Download
1 / 55
560 likes | 782 Views
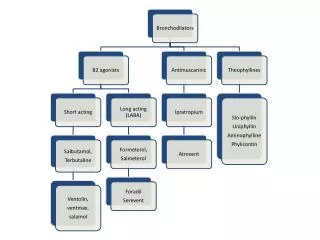
Pharmacology of reproduction. ORAL CONTRACEPTION. ORAL STEROID CONTRACEPTION. COMBINED(COC) x only PROGESTIN (POP) x POSTCOITAL (PCC) efficacy- Pearl index 0,5 - 1 (COC), 0,5 - 4 (POP) ONE PHASE – stable estrogen ( ethinylestradiol ) + stable progestin (derivát 19-nortestosteronu )

E N D
ORAL STEROID CONTRACEPTION • COMBINED(COC) x only PROGESTIN (POP) x POSTCOITAL (PCC) • efficacy- Pearl index 0,5 - 1 (COC), 0,5 - 4 (POP) • ONE PHASE – stable estrogen (ethinylestradiol ) + stable progestin (derivát 19-nortestosteronu ) • TWO PHASES – stable estrogen + 2 doses of progestin • THREE PHASES - 2-3 doses of estrogen + 3 rising doses of progestin
ORAL CONTRACEPTION - II • ethinylestradiol - 20 - 50g (+progestin: levonorgestrel, norgestimat …) • 1 tbl 21 days – 7-days break - pseudomenstruation bleeding • MECHANISM OF ACTION • inhibition of ovulation (progestin), estrogen cycle frequency + cervical mucous changes (pentr. of spermia). + disturbed indometrial quality ( nidation) + motility of ovarian tubes • OTHEr EFFECTS: • ovaria (function,), uterus (changes in cervical mucus, atrophy, bleeding), breast (stimulation of proliferation, enlargment),CNS (excitability:E-,P-), endocrine fcion (GnRH, ACTH), hemocoagulation (f.VII, VIII, IX, X), liver (syntetic fction), lipid metabolism (LDL,HDL), glucose met. (insulin),
ORAL CONTRACEPTION - III • EFFECTS - BENEFITS • profylaxis of ectopic. gravidity, PID, anemia, PMS, dysmenorhea, endometrial and ovarial ca, benign mastopathy, bone mass • RISKS • KI: pregnancy, lactation, thromboembolic dis., liver dis, hypertension, smoking35 let,breast ca, gynekol. bleeding of unknown etiology, migrena • AE: tension in breast, depresion, libido disorders, headache, TE events, GIT (nausea) • DI: ! inductors of enzymes (carbamazepin, phenytoin, rifampicin)
Emergency Contraception Definition: emergency contraceptives are methods a woman can use after intercourse to prevent pregnancy Methods: • Plan B − the only dedicated product marketed specifically for emergency contraception • Off-label use of progestin-only contraceptive pills • Off-label use of combination estrogen-progestin pills • Insertion of a copper-releasing IUD
Emergency Contraception Indications for use: • contraceptive failure (condom broke, pills forgotten) • error in withdrawal or periodic abstinence • rape • any unintended “sperm exposure” Contraindications: • pregnancy EC could prevent about ½ of unintended pregnancies − 1.5 million pregnancies in the U.S. every year.
Emergency Contraception: Plan B Contents: 750 µg levonorgestrel per pill Directions: Take the first tablet as soon as possible within 72 hours after unprotected intercourse. Take the second tablet 12 hours later. The sooner Plan B is taken, the better. It can be taken up to 120 hours after intercourse. If taken within 72 hours as directed, Plan B reduces the risk of pregnancy from a single act of intercourse by 89%. ≈ $35.00 per pack
• Disruption of development and maturation of ovarian follicles • Disruption of egg maturation and ovulation • Interference with corpus luteum function • Alteration of cervical mucus, blocking sperm transport • Disruption of development of the zygote, morula, & blastocyst • Impaired transport in the fallopian tube & uterine cavity • Interference with development of the endometrium to impede implantation Emergency Contraception: Plan B Mechanisms of Action
When does pregnancy start??? The American College of Obstetricians and Gynecologists (ACOG), the Food and Drug Administration (FDA), and the National Institutes of Health (NIH) have defined implantation as the beginning of pregnancy. If fertilization has occurred, implantation starts about 7 days after ovulation. Plan B disrupts the events leading up to implantation. After implantation, it has no effect.
Emergency Contraception: Plan B Is Plan B an “abortion pill?” No. The oral abortifacient is RU-486 (mifepristone, Mifeprex) which is an antiprogestin that blocks the effects of progesterone by binding to its receptors. It is usually given in combination with misoprostol (Cytotec) to medically induce abortion in gestational ages up to 49 days after LMP. If implantation has occurred, Plan B will do nothing.
Emergency Contraception Alternatives to Plan B: 20 tablets of a progestin-only pill (e.g., Micronor) x 2 doses, 12 hours apart 2 doses of a combined estrogen-progestin pill, 12 hours apart Alesse 5 pink pills (100 µg EE + 500 µg levonorgestrel) Triphasil 4 yellow pills (120 µg EE + 500 µg levonorgestrel) Ovral 2 white pills (100 µg EE + 500 µg levonorgestrel) If you give estrogen, give an antiemetic also!
Emergency Contraception Standards of care: • providing information • providing post-coital treatment • providing advance Rx “Every woman, every visit.” − ACOG www.NOT-2-LATE.com 1-888-NOT-2-LATE
MEN HORMONAL CONRACEPTION • low doses of testosterone • GnRH antagonists • 17-methyl-19-nortestosteron (MENT)
THALIDOMIDE • Thalidomide (Contergan) - 1956 –morning nausea of pregnant women • in 28 countries 100 000 kg of thalidomide, • malformed more than 10.000 children - phocomelie • teratogenic dose in men very low ! (0,1 mg/kg) • tested several animal species (instead of rabbitt) - 20-300 mg/kg • only one dose is sufficient 50-100 mg in critical period (21.-36. after conception)
A teratogen is an agent that can produce a permanent alteration of structure or function in an organism exposed during embyronic or fetal life.
Many agents can produce a teratogenic effect under some circumstances.
Factors That Influence Teratogenicity • Nature of the agent • Dose • Route • Frequency of exposure • Duration of exposure
Factors That Influence Teratogenicity • Gestational timing • Concurrent exposures • Concurrent illness • Genetic susceptibility • Mother • Fetus
Principal Mechanisms of Teratogenesis • Cell growth or proliferation • Cell death • Cell migration • Cell and tissue interactions • Disruptions
Mutagenesis • Principal mechanisms • Gene mutation • Chromosomal abnormalies • Before or after conception • Males and females both affected
Birth Defects in Childhood Teratogens 10% Multifactorial 42% Monogenic 8% Unknown 37% Chromosomal 3% Baird et al. AJHG 42:677, 1988
Birth Defects in Childhood Teratogens
Birth Defects Caused By Teratogenic Exposures Are Preventable.
Prevention of Birth Defects Caused by Teratogenic Exposures is an Important Public Health Problem.
Public Health Concerns • Prevention of known teratogenic exposures • Alcohol • Infectious diseases • Isotretinoin, thalidomide
Public Health Concerns • Occupational exposures • Environmental exposures • Drugs of abuse • Medications
Medications • Over-the-counter medicines • Herbals and dietary supplements • Prescription drugs
Medications • Frequently used by pregnant women • Biologically active • Taken systemically • Taken in high doses • Information about teratogenicity very limited
Teratogenic Risk of 468 Drugs Approved 1980-2000 Lo & Friedman, 2002
Teratogenic Risk of 468 Drugs Approved 1980-2000 • 11 (2.4%) of treatments pose a “small”, “moderate” or “high” teratogenic risk • On average, 6.0 ± 4.1 years after FDA approval required to recognize risk in humans Lo & Friedman, 2002
Teratogenic Risk of 468 Drugs Approved 1980-2000 • 30 (6.4%) of treatments unlikely to pose a risk in human pregnancy • On average, 9.1 ± 4.5 years after FDA approval required to show safety in humans Lo & Friedman, 2002
Animal teratology studies are valuable but false positives and false negatives do occur.
Animal Teratology Studies: False Positives • Chlorpheniramine • Hydroxyzine • Propoxyphene
Animal Teratology Studies: False Negatives • Captopril, enalapril • Carbimazole, methimazole • Misoprostol
Lack of Knowledge Is a Problem • Pregnant women may not receive treatments that benefit their own health or that of the fetus • Exposures that really do pose a risk remain unrecognized
Lack of Knowledge Is a Problem • Women may be advised or choose to terminate pregnancy to avoid risk • Labeling tends to provoke anxiety, often unnecessarily
Public Health Priorities • Characterizing teratogenic risks of important exposures • Prevention of exposures that are known to be teratogenic • Recognition of pregnancies at high risk