ESWL for Ureteric Stones
20 likes | 421 Views
No. 130. ESWL for Ureteric Stones Superior u reteric s tone c learance with shockwave l ithotripsy u nder a naesthesia : A r eview of 106 cases ). D.R. Lenaghan , C. Kaiser, M. Salvatore, J.R . Goad , A.H. Clarke

ESWL for Ureteric Stones
E N D
Presentation Transcript
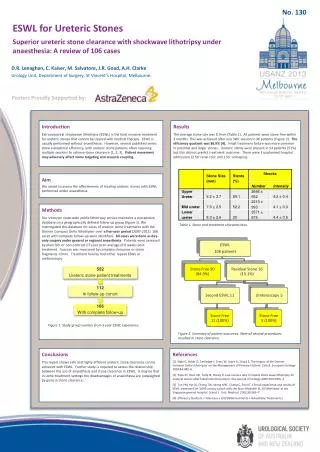
No. 130 ESWL for Ureteric Stones Superior ureteric stone clearance with shockwave lithotripsy under anaesthesia: Areview of 106 cases) D.R. Lenaghan, C. Kaiser, M. Salvatore, J.R. Goad, A.H. Clarke Urology Unit, Department of Surgery, St Vincent’s Hospital, Melbourne, Posters Proudly Supported by: Introduction Extracorporeal shockwave lithotripsy (ESWL) is the least invasive treatment for ureteric stones that cannot be cleared with medical therapy. ESWL is usually performed without anaesthesia. However, several published series show suboptimal efficiency, with ureteric stone patients often requiring multiple sessions to achieve stone clearance [1, 2, 3]. Patient movement may adversely affect stone targeting and acoustic coupling. Results The average stone size was 8.7mm (Table 1). All patients were stone free within 3 months. This was achieved after one SWL session in 90 patients (Figure 2). The efficiency quotient was 86.9% [4]. Initial treatment failure was more common in proximal and larger stones. Ureteric stents were present in 54 patients (51%) but this did not predict treatment outcome. There were 3 unplanned hospital admissions (2 for renal colic and 1 for urosepsis). Aim We aimed to assess the effectiveness of treating ureteric stones with ESWL performed under anaesthesia. Methods Our Victorian state-wide public lithotripsy service maintains a prospective database on a geographically defined follow-up group (figure 1). We interrogated this database for cases of ureteric stone treatments with the Dornier Compact Delta lithotripter over a five-year period (2007-2012). 106 cases with complete follow-up were identified. All cases were done as day-only surgery under general or regional anaesthesia. Patients were assessed by plain film or non-contrast CT scan at an average of 6 weeks post-treatment. Success was measured by complete clearance or stone fragments <2mm. Treatment failures had either repeat ESWL or ureteroscopy. Table 1. Stone and treatmentcharacteristics. Figure 1. Study group number from 5 year ESWL experience. Figure2. Summary of patient outcomes. Note all second procedures resulted in stone clearance. . Conclusions This report shows safe and highly efficient ureteric stone clearance can be achieved with ESWL. Further study is required to assess the relationship between the use of anaesthesia and stone clearance in ESWL. It may be that in some treatment settings the disadvantages of anaesthesia are outweighed by gains in stone clearance.. References [1] Nabi G, Baldo O, Cartledge J, Cross W, Joyce A., Lloyd S. The Impact of the Dornier Compact Delta Lithotriptor on the Management of Primary Ureteric Calculi. European Urology 2003;44:482–6. [2] Pace KT, Weir MJ, Tariq N, Honey R. Low success rate of repeat shock wave lithotripsy for ureteral stones after failed initial treatment. The Journal of Urology 2000;164:1905–7. [3] Tan YM, Yip SK, Chong TW, Wong MYC, Cheng C, Foo KT. Clinical experience and results of ESWL treatment for 3,093 urinary calculi with the StorzModulith SL 20 lithotripter at the Singapore general hospital. Scand. J. Urol. Nephrol. 2002;36:363–7. [4] Efficiency Quotient = %Success x 100/(%Retreatments + %Auxilliary Treatments)