Download
1 / 1
10 likes | 171 Views
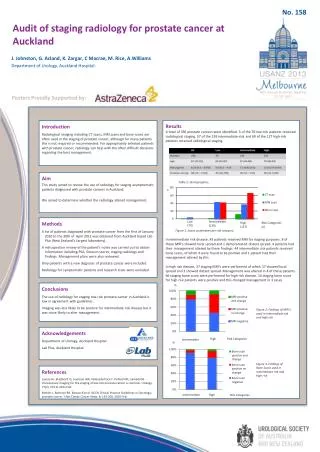
No. 158. Audit of staging r adiology for prostate c ancer at Auckland ). J. Johnston, G. Acland, K. Zargar, C Macrae, M. Rice, A.Williams Department of Urology, Auckland Hospital. Posters Proudly Supported by:. Results

E N D
No. 158 Audit of staging radiology for prostate cancer at Auckland) J. Johnston, G. Acland, K. Zargar, C Macrae, M. Rice, A.Williams Department of Urology, Auckland Hospital. Posters Proudly Supported by: Results A total of 336 prostate cancers were identified. 5 of the 70 low-risk patients received radiological staging. 57 of the 139 intermediate-risk and 69 of the 127 high-risk patients received radiological staging. In intermediate risk disease, 43 patients received MRI for staging purposes. 8 of these MRI’s showed local spread and 1 demonstrated distant spread. 4 patients had their management altered by these findings. 44 intermediate risk patients received bone scans, of which 4 were found to be positive and 1 patient had their management altered by this. In high risk disease, 37 staging MRI’s were performed of which 17 showed local spread and 3 showed distant spread. Management was altered in 4 of these patients. 66 staging bone scans were performed for high risk disease. 14 staging bone scans for high risk patients were positive and this changed management in 3 cases Introduction Radiological imaging including CT scans, MRI scans and bone scans are often used in the staging of prostate cancer, although for many patients this is not required or recommended. For appropriately selected patients with prostate cancer, radiology can help with the often difficult decisions regarding the best management. Aim This study aimed to review the use of radiology for staging asymptomatic patients diagnosed with prostate cancers in Auckland. We aimed to determine whether the radiology altered management. Table 1: Demographics. n Low (70) Intermediate (139) Methods A list of patients diagnosed with prostate cancer from the first of January 2010 to the 30th of April 2012 was obtained from Auckland based Lab Plus (New Zealand’s Largest laboratory). A retrospective review of the patient’s notes was carried out to obtain information including PSA, Gleason scores, staging radiology and findings. Management plans were also reviewed. Only patients with a new diagnosis of prostate cancer were included. Radiology for symptomatic patients and research trials were excluded Risk Categories (n) High (127) Figure 1: Scans undertaken per risk category % Conclusions The use of radiology for staging low-risk prostate cancer in Auckland is low in agreement with guidelines. Imaging was less likely to be positive for intermediate risk disease but it was more likely to alter management. Figure 2: Findings of MRI’s used in intermediate risk and high risk Acknowledgements Department of Urology, Auckland Hospital Lab Plus, Auckland Hospital High Risk Categories Intermediate % Figure 3: Findings of Bone Scans used in intermediate risk and high risk References Lavery HJ, Brajtbord JS, Levinson AW, Nabizada-Pace F, Pollard ME, Samadi DB. Unnecessary imaging for the staging of low-risk prostate cancer is common. Urology. 77(2); 274-8, 2011 Feb. Mohler J, Bahnson RR, Boston B et al. NCCN Clinical Practice Guidelines in Oncology; prostate cancer. J Nat Compr Cancer Netw. 8; 162-200, 2010 Feb. Intermediate High Risk Categories