ACUTE SPINAL CORD LESSION
290 likes | 500 Views
ACUTE SPINAL CORD LESSION. MEITI FRIDA DEPARTMENT OF NEUROLOGY FACULTY OF MEDICINE ANDALAS UNIVERSITY. ANATOMY OF SPINE AND SPINAL CORD. The spine has three major components : the spinal column (bones and discs) neural elements (the spinal cord and nerve roots)

ACUTE SPINAL CORD LESSION
E N D
Presentation Transcript
ACUTE SPINAL CORD LESSION MEITI FRIDA DEPARTMENT OF NEUROLOGY FACULTY OF MEDICINE ANDALAS UNIVERSITY
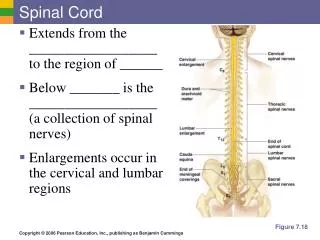
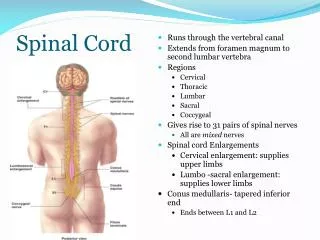
ANATOMY OF SPINE AND SPINAL CORD The spine has three major components: • the spinal column (bones and discs) • neural elements (the spinal cord and nerve roots) • supporting structures (muscles and ligaments) The spinal column consists of: • seven cervicalvertebrae (C1–C7) i.e. neck • twelvethoracic vertebrae (T1–T12) i.e. upper back • five lumbar vertebrae (L1–L5) i.e. lower back • five bones (that are joined, or "fused," together in adults) to form the bony sacrum • three to five bones fused together to form the coccyx or tailbone
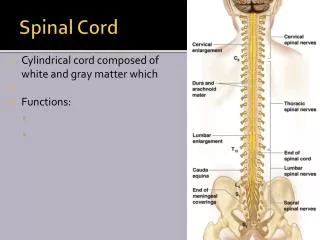
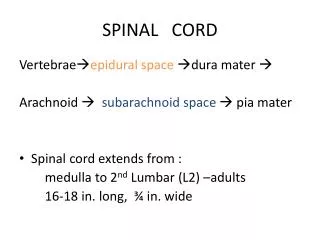
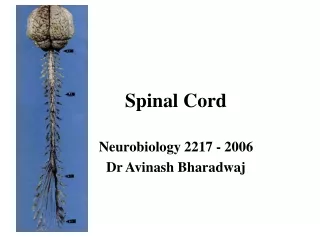
Adult spinal cord: • Inside vertebral canal • 31 segments, each associated with a pair of dorsal root ganglia • Extends to L1/ L2 (Conusmedularis) • Caudaequina - origin of spinal nerves extending inferiorly from conusmedullaris
Spinal Meningen Three membranes surround all of CNS 1) Dura mater - "tough mother", strong 2) Arachnoid- spidery looking, carries blood vessels, etc. Subarachnoid space 3) Pia mater - adheres tightly to surface of spinal cord 3) Pia mater 2) Arachnoid 1) Dura mater
Organization of Cord Cross Section Gray matter posterior - somatic and visceral sensory nuclei anterior (and lateral) gray horns – somatic and visceral motor control gray commissures - axons carrying information from side to side White matter posterior white column - anterior white column lateral white column anterior white commissure Functions ascending tracts - sensory toward brain descending tracts - motor from brain
Vascular anatomy - Anterior spinal artery • Anterior spinal artery originates in upper cervical region, from anterior spinal branches of vertebral artery. • 6-10 anterior radicular arteries contribute to it throughout its length. • Supplies anterior two thirds of cord, via central branches and penetrating branches of pial plexus
Vascular anatomy – posterior spinal artery • Run along posterolateral cord • Sometimes discontinuous • Originates from verterbral artery • Has contribution from 10-23 posterior radicular a. • Supplies posterior one third of cord
Acute lession of spinal cord • Traumatic spinal cord injury • Vascular Myelopathies • Infectious Myelopathies • Inflammatory Myelopathies
Traumatic spinal cord injury Mechanism of injury • Flextion and flextion-rotation injury • Compression injury • Hyperextention injury Level of injury • Quadriplegia : injury in cervical region all 4 extremities affected • Paraplegia : injury in thoracic, lumbar or sacral segments 2 extremities affected
Complete and Incomplete Spinal Cord Syndromes can be classified into either complete or incomplete categories • Complete – characterized as complete loss of motor and sensory function below the level of the traumatic lesion • Incomplete – characterized by variable neurological findings with partial loss of sensory and/or motor function below the lesion
Spinal Shock • An immediate loss of reflex function, called areflexia, below the level of injury • Signs: • Slow heart rate • Low blood pressure • Flaccid paralysis of skeletal muscles • Loss of somatic sensations • Urinary bladder dysfunction • Spinal shock may begin within an hour after injury and last from several minutes to several months, after which reflex activity gradually returns
Brown-Sequard Syndrome(Special Form of Spinal Cord Injury) • Results from an injury to only half of the spinal cord and is most noticed in the cervical and thoracal region • Often caused by spinal cord penetrating trauma • Motor loss is evident on the same side as the injury to the spinal cord • Sensory loss is evident on the opposite side of the injury location (pain and temperature loss) • Bowel and bladder functions are usually normal • Person is normally able to walk although some bracing or stability devices may be required
ASIA Impairment Scale of spinal cord injury ASIA – American Spinal Injury Association : A – Complete: no sensory or motor function preserved in sacral segments S4 – S5 B – Incomplete: sensory, but no motor function in sacral segments C – Incomplete: motor function preserved below level and power graded < 3 D – Incomplete: motor function preserved below level and power graded 3 or more E – Normal: sensory and motor function normal
ATLS principles • Airway; protect spine • Breathing • Circulation • Disability • Expose patient • Treat • Secondary survey
Pharmacologic Therapy • Option: Methylprednisolone • NASCIS II (1992) • 30mg/kg IV loading dose + 5.4 mg/kg/hr (over 23hrs) effective if administered within 8 hours of injury • NASCIS III (1997) • If initiated < 3hrs continue for 24 hrs, if 3-8 hrs after injury, continue for 48hrs (morbidity higher - increased sepsis and pneumonia)
Vascular Myelopathies • Spinal Cord Ischemia • Spinal Hemorrhage Spinal Cord ischemia • In most cases Sensory features ( pain ) emerge first , followed by weakness within minutes or hours • Pain often follows radicular pattern ( common presentation ) • Maximum weakness is observed within 12 hrs of onset • Lower thoracic and lumbar spinal levels are most commonly affected • Urinary retention : in acute phase Involuntary voiding or defecation : associated with onset of ischemic insult
Spinal Cord Hemorrhage • Spinal cord dysfunction – due to hemorrhage into Sub arachnoid space Sub dural space Epidural space • Onset : Sudden & Painful • Triggers : Trauma Bleeding diatheses Vascular malformations
Investigations : • CSF Analysis : usually normal can be xanthochromic raised protein • MRI • Contrast enhanced CT scan with sagittal / coronal reformatting is useful in pts who cannot undergo MRI • MR Angiography • Selective Spinal Angiography using Digital Substraction Techniques Treatment : • SCH is surgical emergencies • Immediate surgery • Laminectomy and clot evacuation • Angiographically directed embolization of vascular malformation
Infectious Myelopathies Virus • Enteroviruses(poliovirus, coxsackie virus, and enterovirus 71), Flaviviruses (West Nile virus and Japanese encephalitis virus) have been known to target the gray matter (Anterior horn cells) producing acute lower motor neuron disease • CMV, VZV, HSV I &II, HCV, and EB • HIV Bacterial • Mycoplasma (acute and post infectious), Listeriamonocytogenes • TB • Lyme disease Schistosomiasis (in endemic areas)
Clinical features of infectious process • Fever • Meningismus • Encephalopathy • Rash • Lymphadenopathy • Known systemic infection • Immunocompromised status • Known exposure to infectious agent
Inflammatory Myelopathies • Acute Disseminated Encephalomyelitis • Transverse Myelitis Acute Disseminated Encephalomyelitis • Characterized by acute to subacute onset of fever, meningismus, encephalopathy and multifocal symptoms & signs of CNS dysfunction • More common in children • Recent vaccination or systemic infection is noted in ½ of cases • Brain MRI reveals numerous medium to large size , fairly symmetrical subcortical white matter lesions often with involvement of deep gray matter
Transverse Myelitis (TM) • Immune-mediated process results in neural injury to the spinal cord • Varying degrees of weakness, sensory alterations and autonomic dysfunction • Up to half of idiopathic cases will have a preceding respiratory or gastrointestinal illness
Treatment of Myelitis • Acute myelitis attacks are typically treated with IV Corticosteroids Methyl prednisolone • Resistant cases : Plasmapheresis • Very severe attacks : combination of Corticosteroids, Plasmapheresis, Cyclophosphamide • No evidence supports use of IV Ig in inflammatory myelitis
Neoplastic & ParaneoplasticMyelopathies • Most primary tumors of cord do not cause acute myelitis syndromes • Lymphoma is the only exception – causes a subacutemyelopathy - corticosteroid responsive • Breast carcinoma : antiamphiphysin antibodies and severe spastic myelopathy • Ovarian and Non small cell lung cancer : glutamic acid decarboxylase 65 autoantibodies causing stiff man like syndrome with brain stem features and ataxia