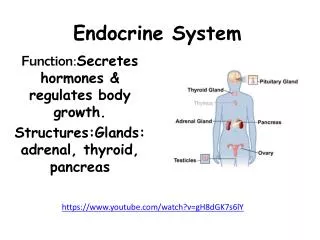
Endocrine System
Endocrine System. PART II. DISORDERS OF THE GONADS. NOONAN SYNDROME. SHORT STATURE, webbing of the neck, pectus carinatum / excavatum , cubitus valgus , R sided congenital HD, characteristic facies .

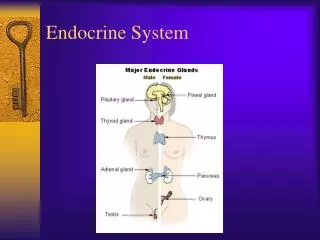
Endocrine System
E N D
Presentation Transcript
Endocrine System PART II
NOONAN SYNDROME • SHORT STATURE, webbing of the neck, pectuscarinatum/excavatum, cubitusvalgus, R sided congenital HD, characteristic facies. • Hypertelorism, epicanthus, downward slanted palpebral fissures, ptosis, micrognathia, ear abnormalities • Mean IQ 86 (53-127) • Verbal IQ> performance IQ
NOONAN SYNDROME • PULMONARY VALVULAR STENOSIS, HYPERTROPHIC CM, ASD • Hepatosplenomegaly, low clotting factors XI XII, ALL, CML • CRYPTORHIDISM, SMALL TESTES, hypogonadal or normal • Delayed puberty (2yrs), ADULT HEIGHT 2nd DECADE, usually reaches the lowest limit of the normal population • PRENATAL DX: Normal karyotype, edema, hydrops and short femur length • TREATMENT: HUMAN GH
KLINEFELTER SYNDROME • 1/500 MALES: 47,XXY • ALL BOYS WITH MR and in children with PSYCHOSOCIAL, LEARNING, or SCHOOL ADJUSTMENT problems • Tall, slim, underweight, long legs, body habitus can vary markedly • Testes tend to be small for age, phallus tends to be smaller than average, cryptorchidism or hypospadias may occur in a few patients; SPERMATOGENIC ARREST and SERTOLI CELL PREDOMINANCE • GYNECOMASTIA (80%) • Height tends to be increased
12-yr-old boy with 48,XXXY/49,XXXXY mosaicism who has prognathism, epicanthal folds, scoliosis, small testes, severe mental retardation, clinodactyly, and radioulnarsynostoses
KLINEFELTER SYNDROME • Increased incidence of pulmonary disease, varicose veins, cancer of the breast • Male breast cancer (7.5%), Mediastinal GCT, Leukemia, Lymphoma. Higher cancer risk (RR 2.7): 15-30y age group
KLINEFELTER SYNDROME • Replacement therapy • Long-acting TESTOSTERONE preparation • 11-12 yrs of age • ENANTHATE ESTER 25-50mg IM q3-4w, 50mg increments q6-9mo until a maintenance dose for adults achieved (200-250mg q3-4w) • TESTOSTERONE PATCHES/GEL • Rapid increase in prostate volume and PSA levels
HYPOGONADOTROPIC HYPOGONADISM in the MALE (SECONDARYHYPOGONADISM) • Deficiency of LH or FSH, or both • Primary defect: anterior pituitary/ hypothalamus – deficiency of GnRH • N testes, prepubertal • KALLMAN SYNDROME - +anosmia/hyposmia • Xlinked mutation KAL gene – failure of the olfactory axons and GnRH-expressing neurons to migrate from their common origin in the olfactory placode to the brain • TESTOSTERONE ENANTHATE 100mg IM qMo for 4-6mo increase in signs of secondary sexual characteristics, increase in growth velocity • hCG 500-1000IU, SC or IM, 3x/wk growth of testes and spermatogenesis • human menopausal gonadotrophin 37.5-150 IU, 3x/wk, may require 2yrs of tx
PSEUDOPRECOCITY resulting from Tumors of the testes • Leydig Cell Tumors – REINKE CRYSTALLOIDS • Adrenal Rest Tumors • bilateral • FRAGILE X SYNDROME • B Testicular enlargement MACROORCHIDISM, 40-50mL
GYNECOMASTIA • TRUE vs PSEUDOGYNECOMASTIA (adipose) • ESTROGEN-ANDROGEN IMBALANCE • Aromatase • Treatment: Reassurance • Medical: Anastrozole (Ar In) 1mg = placebo • Surgical: Removal ENDOSCOPICALLY ASSISTED TRANSAXILLARY REMOVAL
HYPOFUNCTION OF THE OVARIESTURNER SYNDROME • Sexual infantilism, webbed neck, cubitusvalgus • Complete or partial absence of second X chr • BIRTH: edema of dorsum of hands & feet, loose skin folds at the nape. LOW BW and DECREASED LENGTH • CHILDHOOD: webbing of the neck, low posterior hairline, small mandible, prominent ears, epicanthal folds, high arched palate, broad chest, cubitusvalgus, hyperconvex fingernails • SHORT STATURE (US MAH: 143-144cm), MPH
Turner syndrome in a 15-yr-old girl exhibiting failure of sexual maturation, short stature, cubitusvalgus, and a goiter. There is no webbing of the neck. Karyotyping revealed 45,X/46,XX chromosome complement
TURNER SYNDROME • Isolated nonstenotic bicuspid aortic valves, aortic coarctation, AS, MVP • Pelvic kidney, horseshoe kidney, double collecting system, complete absence of 1kidney, UPJ obstruction • Autoimmune thyroid disease • IBD: Chron disease and UC • Sternal malformations • Recurrent Bilateral OM, SNH defects
TURNER SYNDROME • Chromosomal Analysis • Ultrasonography • Plasma Gn: FSH • Thyroid antiPOAb, T4, TSH • Treatment: RECOMBINANT hGH • Replacement E2 Therapy • Conjugated estrogen 0.3-0.625mg • Micronized E2 0.5mg daily x3-6mo
CONGENITAL ADRENAL HYPERPLASIA • Ambiguous genitalia • 21-OH deficiency
Cholesterol P450scc 3(B)HSD P450c21 P450c11 P450c11 P450c11 Pregnelonone Progesterone DOC Corticosterone 180H Corticosterone Aldosterone P450c17 P450c17 3(B)HSD P450c11 P450c21 170H Pregnenolone 170H Progesterone 11 Deoxycortisol Cortisol 3(B)HSD 17(B)HSD P450aro DHEA Androstenedione Testosterone Estradiol
CONGENITAL ADRENAL HYPERPLASIA • SALT WASTING • Progressive weight loss, anorexia, vomiting, dehydration, weakness, hypOtension, hypOglycemia, hypOnatremia, hypErkalemia • 2 Wks of age • GLUCOCORTICOID 15-20mg/m²/24 • FLUDROCORTISONE 0.1-0.3mg/day
WAGRWILMS TUMOR, ANIRIDIA,GENITOURINARY MALFORMATIONS, RETARDATION • Deletion c11p13 (aniridia gene PAX6, WT1) • 46,XY males have genital abnormalities • Cryptorchidism • Virilization
ANDROGEN INSENSITIVITY SYNDROMES • 46,XY • Phenotypic females (COMPLETE AIS) to males with various ambiguous genitals and undervirilization (PARTIAL) • Complete: female at birth, F external genitals, blind vaginal pouch, absent uterus, FT remnants, intraabdominal testes. • Puberty: N breast development, female habitus, menstruation does not occur, absent sexual hair • Adult height same with N males • N testosterone and DHT levels • Testicular removal (seminoma); ESTROGEN
Type 1 DM • IDDM, juvenile diabetes • Low/ absent levels of endogenously produced insulin and dependence on exogenous insulin to prevent DKA • 4 stages: • Preclinical β-cell autoimmunity with progressive defect of insulin secretion • Onset of clinical diabetes • Transient remission “honeymoon period” • Established diabetes associated with acute and chronic complications and decreased life expectancy
Type 1 DM • Onset: 7-15 y/o • Autoimmune destruction
T2 DM • Usually obese but are not insulin dependent • NIDDM, adult-onset DM, MODY • More insidious • Excessive weight gain, fatigue • ACANTHOSIS NIGRICANS
T2 DM CRITERIA • OVERWEIGHT (BMI>85th % A,S; WFH>85th %; Wt>120% of ideal for ht) PLUS: Any 2 of the ff: • FH T2DM in 1st or 2nd degree relative • Race/Ethnicity • Signs of Insulin Resistance or conditions associated with insulin resistance (AN, hypertension, dyslipidemia, PCOS) • Age of initiation: age 10yrs or at onset of puberty if puberty occurs at a younger age • Frequency: every 2 yrs • Test: FPG preferred
Diagnosis • “inappropriate polyuria in any child with dehydration, poor weight gain, or the flu” • RBS>200mg/dL (11.1 Treatment Insulin therapy prepubertal 0.7 U/Kg/d midpuberty 1.0 U/Kg/d end 1.2 U/Kg/d Nutritional Education Improved Exercise Level
Long Term Complications • Microvascular • Retinopathy • Nephropathy • Macrovascular • CAD • CVD • PVD • Neuropathies • Peripheral • Autonomic
TRANSIENT DM of the NEWBORN • 1st week of life • SGA • Hyperglycemia, pronounced glycosuria • Severe dehydration, metabolic acidosis but with only minimal or no ketonemia/ketonuria • 1-2U/Kg/24h intermediate actingINSULIN insulin
Glycogen Storage Disease type I (GLUCOSE-6-PHOSPHATASE/ TRANSLOCASE/ VON GIERKE DISEASE) • Neonatal period: Hypoglycemia and lactic acidosis • 3-4mo: hepatomegaly, hypoglycemic seizures • Doll like faces with fat cheeks, relatively thin extremities, short stature, protruberant abdomen, enlarged kidneys • Hypoglycemia, Lactic Acidosis, Hyperuricemia, Hyperlipidemia • NORMAL transaminases • Tx: NGT infusion of glucose/ oral uncooked cornstarch
Glycogen Storage Disease type III (DEBRANCHER DEFICIENCY) • Deficiency of glycogen debranching enzyme activity • Hepatomegaly, hypoglycemia, short stature, variable skeletal myopathy, variable CM • BOTH LIVER AND MUSCLE INVOLVEMENT (IIIa) • LIVER (IIIb) • ELEVATION OF LIVER TRANSAMINASES • HEPATOCELLULAR CARCINOMA • Tx: Frequent meals with high in CHO, high CHON diet
GSDIIIb Growth and development in a patient with type IIIb glycogen storage disease. The patient has debrancher deficiency in liver but normal activity in muscle. As a child, he had hepatomegaly, hypoglycemia, and growth retardation. After puberty, he no longer had hepatomegaly or hypoglycemia, and his final adult height is normal. He had no muscle weakness or atrophy; this is in contrast to type IIIa patients, in whom a progressive myopathy is seen in adulthood.
Glycogen Storage Disease type IV(Branching Enzyme Deficiency/ Amylopectinosis/ Andersen Disease) • Accumulation of an abnormal glycogen with poor solubility • Fewer branch points • Progressive cirrhosis of the liver • 1st 18 mo: hepatosplenomegaly, FTT • Cirrhosis progresses to portal HPN, ascites, esophagealvarices, liver failure • Death by 5 y/o • NO SPECIFIC TX, poor prognosis
Glycogen Storage Disease type II (LYSOSOMAL ACID a1-4-GLUCOSIDASE DEFICIENCY/ POMPE DISEASE) • Lysosomal glycogen accumulation in multiple tissues, cardiac, skeleletal, SMOOTH MUSCLE CELLS • Myopathy, “floppy infant appearance”, feeding difficulties, macroglossia, hepatomegaly, hypertrophic CM • Slowly progressive proximal muscle weakness with truncal involvement • LE> UE • Lab: elevated CK, AST, LDH; muscle def a-glucosidase • Tx: Supportive/ Palliative
GALACTOSEMIA (Galactose-1-Phosphate UridylTransferase Deficiency) • 2nd half of the 1st week of life • Accumulation of galactose-1-phosphate kidney/liver/brain injury • Jaundice, hepatomegaly, vomiting, hypoglycemia, convulsions, lethargy, irritability, feeding difficulties, FTT, aminoaciduria, nuclear cataracts, vitreous hge, hepatic failure, liver cirrhosis, ascites, splenomegaly, mental retardation. • Dx: Reducing substance in urine • Tx: Elimination of galactose from the diet
MUCOPOLYSACCHARIDOSIS IHURLER DISEASE • 6 to 24 months old • Hepatosplenomegaly, coarse facial features, corneal clouding, large tongue, prominent forehead, joint stiffness, short stature and skeletal dysplasia, developmental delay
MUCOPOLYSACCHARIDOSIS IIHUNTER DISEASE • Almost exclusively in MALES • Same with Hurler EXCEPT for LACK OF CORNEAL CLOUDING and somewhat SLOWER progression of somatic and CNS deterioration
MUCOPOLYSACCHARIDOSIS • Treatment • BM transplantation • CORD BLOOD transplantation • Enzyme replacement