Download
1 / 58
640 likes | 803 Views
Pharmacology for Pain and Analgesia. Dept of Pharmacology Shi-Hong Zhang ( 张世红 ) shzhang713@zju.edu.cn. What is pain.

E N D
Pharmacology for Pain and Analgesia Dept of Pharmacology Shi-Hong Zhang (张世红) shzhang713@zju.edu.cn
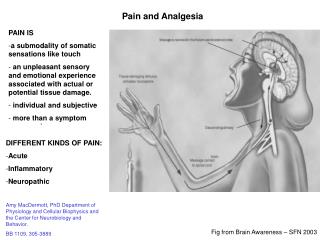
What is pain An unpleasant sensory or emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is always subjective. Each individual learns the application of the word through experiences related to injury in early life. It is unquestionably a sensation in a part of the body, but it is also unpleasant, and therefore also an emotional experience. Many people report pain in the absence of tissue damage or any likely pathophysiological cause; usually this happens for psychological reasons. There is no way to distinguish their experience from that due to tissue damage, if we take this subjective report…… IASP. Pain 1979(6)249-252
Physiology of Pain Pain sensation First pain:sharp, pricking, well defined,A fibers Second pain:dull, aching, poorly localized, C fibers
Chronic Pain Types and reasons Neuropathic pain Inflammatory pain Bone cancer pain Fibromyalgia Migraine Psychogenic pain
Chronic Pain Mechanisms: Peripheral input Central sensitization
Plus dysfunction in inhibitory systems, including opioids, cannabinoids, norepinephrine, adenosine…
Analgesics (pain killer) • NSAIDs and other anti-inflammatory drugs • Opiates and morphinomimetics • Some tricyclic antidepressants • Some antiepileptic drugs • Local anesthetics • Others: ketamine, mexiletine, etc
Antipyretic, Analgesic, and Anti-inflammatory Drugs (Non-steroidal anti-inflammatory drugs, NSAIDs)
Phospholipid Bradykinin Angiotensin ⊕ Corticosteroids Phospholipase A2 Arachidonic acid Cyclooxygenase (COX) NSAIDs 5-lipoxygenase PGG2 Prostacyclin(PGI2) hydroperoxidase PGE2 PGF2α PGH2 Leukotrienes Thromboxane A2 Dipyridamole
Characteristics comparison between COX-1 and COX-2
Classification of NSAIDs : Aspirin and other salicylates(阿司匹林及水杨酸类) Aniline derivatives(苯胺类衍生物) Indole derivatives(吲哚类衍生物) Propionic acid derivatives(丙酸类衍生物) Others (烯醇酸类,灭酸类,杂环芳基乙酸类,茚乙酸类,吡唑酮类,以及选择性COX-2抑制剂)
1. Aspirin The mechanism of aspirin: acetylating COX enzyme irreversibly
1. Aspirin 1.1 Actions and therapeutic uses: A Antipyretic and analgesic actions: -- resets the thermostat toward normal and lowers the body temperature by increasing heat dissipation; -- alleviates pain of low to moderate intensity arising from integument, especially with inflammation.
1. Aspirin 1.1 Actions and therapeutic uses: B Anti-rheumatic actions:atlarge dose (4-6 g/d). C Anti-aggregation of platelets and vasoconstriction:at small dose (~100 mg/d), irreversibly inhibits thromboxane production in platelets without markedly affecting PGI2 in the endothelial cells of the blood vessel.
1. Aspirin 1.2 Adverse effects: Gastrointestinal effects:epigastric distress, nausea and vomiting, bleeding, ulcer. Allergic effects: Urticaria (风疹) Bronchoconstriction (aspirin asthma) angioneurotic edema
1. Aspirin 1.2 Adverse effects: Prolonged bleeding time Excessive ventilation: respiratory alkalosis Salicylism (水杨酸反应):toxicity in the CNS (headache, dizziness, nausea, vomiting, tinnitus) Reye’s syndrome: liver and brain injury in children with virus infection
2. Acetaminophen (对乙酰氨基酚) • Slow and prolonged antipyretic and analgesic effects • No obvious anti-inflammation effect • Less stimulation to gastrointestinal tract • Damage of liver and kidney if used for a long time and at high dose
3. Indomethacin(吲哚美辛) • One of the most potent inhibitors of COX • High potency of anti-inflammatory, analgesic, and antipyretic activity • Used for ankylosing spondylitis (强直性脊柱炎SA),Osteoarthritis (骨关节炎OA) and gout (痛风) • Effective in treating patent ductus arteriosus (动脉导管未闭)
3. Indomethacin • High incidence of adverse effects like: central nervous system effect gastrointestinal complaints allergic reactions hematopoietic reactions • Sulindac (舒林酸) and Etodolac (依托度酸) are less toxic and used for OA, RA, SA and acute gout.
4. Propionic acid derivatives (丙酸类) • Anti-inflammatory, analgesic and antipyretic activity • Less gastrointestinal effects • Change platelet function and prolong bleeding time • Used for the treatment of various arthritis and dysmenorrhea (痛经)
5. Inhibitors of TNF- • TNF- is the predominant factor in inflammatory reaction. • Include infliximab, adalimumab and IgG1 • Used for the treatment of rheumatoid arthritis, spondylitis ankylosans (强直性脊柱炎) and other autoimmune diseases.
Crude opium Seeds of opium poppy Collecting resin of opium poppy Opium flowers
1. Classification of opiates • Natural opiates: morphine, codeine, papaverine and thebaine; • Semi-synthetic opiates: hydromorphone, hydrocodone, oxycodone, oxymorphone, desomorphine, diacetylmorphine (Heroin), nicomorphine, dipropanoylmorphine, benzylmorphine and ethylmorphine; • Fully synthetic opioids: fentanyl, pethidine, methadone, tramadol and propoxyphene; • Endogenous opioid peptides: endorphins, enkephalins, dynorphins, and endomorphins.
2. Opioid receptors 2.1 Distribution and physiological effects: A Certain cells in the CNS: Brainstem: mediate respiration, cough, nausea and vomiting, maintain blood pressure, pupillary diameter and control of stomach secretions. Medial thalamus: modulate deep pain that is poorly localized and emotionally influenced.
2. Opioid receptors 2.1 Distribution and physiological effects : A Certain cells in the CNS: Spinal cord: involved in the reception and integration of incoming sensory information and attenuate painful afferent stimulation. Hypothalamus:affect neuroendocrine secretion. Limbic system:influence emotional behavior.
2. Opioid receptors 2.1 Distribution and physiological effects : B Periphery: --- Inhibit the release of excitatory, proinflammatory substances from nerve endings, which contribute to the anti-inflammatory effect of opioids. C Immune cells: immune depression
2. Opioid receptors 2.2 Signal transduction: In the Spinal Cord
2. Opioid receptors In the Brain Stem
3. Opioids Summary of opioid analgesics and antagonists: Strong agonists: fentanyl, heroin, pethidine, methadone, morphine Moderate agonists: codeine Mixed agonist-antagonists: pentazocine Antagonists: naloxone, naltrexone
Mainly agonist action atμreceptors, • but some actions on other receptors • Morphine • Heroin • Codeine • Fentanyl • Agonist action at κreceptors, • with partial antagonist action • at μ receptors • Pentazocine ⊕ ⊕ ⊕ μopioid receptor κ opioid receptor opioid receptor Analgesia Respiratory depression Euphoria/sedation Physical dependence Decreased GI motility Pupil constriction Analgesia Sedation/dysphoria Pupil constriction Analgesia • Antagonist act at μ, κ, receptors • Naloxone • Naltrexone
Efficacy high Addiction/abuse low Morphine Pethidine Methadone Fentanyl Codeine A comparison of the maximum efficacy and addiction/abuse liability of commonly used narcotic analgesics
Time to peak effect Duration of action 20min Morphine Pethidine Fentanyl 4 hours 15min 2 hours 5min 45min Time to peak effect and duration of action of several opioids administered intravenously
4. Morphine 4.1 Pharmacological effects: A Analgesia: - Raises the pain threshold at the spinal cord level, alters nociception in the brain. - Relieves anxiety and fear B Euphoria: - Produces a powerful sense of contentment and well-being by stimulation of the ventral tegmentum.
4. Morphine C Respiration: - Causes respiration depression by reduction of the sensitivity of respiratory center neurons to carbon dioxide. D Depression of cough reflex: - May allow accumulation of secretions and thus lead to airway obstruction and atelectasis (肺不张). -Replaced by other safer antitussives .
4. Morphine E Miosis: - The pinpoint pupil is the characteristic of morphine use, little tolerance. F Emesis: - Causes vomiting by stimulating the CTZ in the medulla but with no unpleasant sensations.
4. Morphine G Sedation: - Causes drowsiness and clouding of mentation, even disrupting sleep H Gastrointestinal effect: - Decreases motility of smooth muscle and increases tone, which causes constipation and increases pressure in the biliary tract (worsens abdominal colic, eg. Sphincter oddi contraction).
4. Morphine I Cardiovascular : - Has no major effects on the cardiovascular system. - Is usually contraindicated in individuals with severe brain injury(because that increased PCO2 induced by respiration depression leads to cerebral vasodilation and consequential increase in cerebral blood flow and intracranial pressure). - Causes postural hypotension sometimes.
4. Pharmacodynamics- morphine J Histamine release: - Causes pruritus, urticaria, sweating, vasodilation and bronchoconstriction. K Hormonal actions: - Inhibits release of LH (黄体生成素). - Increases GRH (促生长激素), ADH (抗利尿激素), PRL (催乳素) M Immune depression
4. Morphine 4.2 Therapeutic uses: A Analgesia: - Used for various pain, especially acute, obstinate constant pain (e.g. burn, cancer pain); - Fixed interval of administration reduces tolerance and dependence; - Severe pain of renal and biliary colic + MR blockers.
4. Morphine B Cardiac asthma: - Acute left ventricular heart failure induces pulmonary edema - Reduces anxiety, cardiac preload and afterload. - Particularly useful for painful myocardial ischemia with pulmonary edema. C Treatment of diarrhea: synthetic surrogates (eg. 地芬诺酯).
4. Morphine D Relief of cough: synthetic antitussives(eg. 右美沙芬) E Premeditate drugs before anesthesia : sedative, anxiolytic, and analgesic properties. For high-risk surgery administered systemically; for local (epidural) anesthesia. Caution: respiratory suppression
4. Morphine 4.3 Adverse effects: -Respiratory depression - Vomiting, constipation, biliary colic - Dysphoria - Allergy-enhanced or postural hypotensive effects - Urinary retention (prostatic hypertrophy) - Elevation of intracranial pressure (head injury) - Immune depression
4. Morphine Tolerance and Physical Dependence • Repeated use produces tolerance to the respiratory depression, analgesic, euphoric and sedative effects, but not to pupil-constricting and constipating effects. • Physical and psychologic dependence readily occur for strong μagonists, especially used on necessities.
4. Morphine Tolerance and Physical Dependence • Withdrawal symptoms: a series of autonomic, motor and psychological response that incapacitate the individual (rhinorrhea, lacrimation, yawning, chills, gooseflesh, hyperventilation, hyperthermia, mydriasis, muscular aches, vomiting, diarrhea, anxiety, and hostility).
Druggy Malformation
4. Morphine 4.4 Contraindications: • Women during labor or lactation • New-born infants • Chronic obstructive pulmonary disease (COPD) • Asthma