Download
1 / 36
390 likes | 417 Views
METASTATIC DISEASE IN BREAST CANCER. Mario Alberto Vásquez-Chaves, MD MsC Tokyo Women´s Medical University June 2011. WHAT IS METASTATIC BRCA?. Anything more distant than ipsilateral Axillar or Internal mammary LNs may PRESENT with distant mets may RECURR outside of this area. INCIDENCE.

E N D
METASTATIC DISEASEIN BREAST CANCER Mario Alberto Vásquez-Chaves, MD MsC Tokyo Women´s Medical University June 2011
WHAT IS METASTATIC BRCA? • Anything more distant than ipsilateral Axillar or Internal mammary LNs • may PRESENT with distant mets • may RECURR outside of this area
INCIDENCE • Between 5-10% metastatic at diagnosis • Majority = women relapsing with metastatic disease • Roughly 40,000 women die each year from metastatic BrCa
SITES OF METASTASES • Bones • Liver • Lungs • Brain • Peritoneal • LAD • Skin
SURVIVAL WITH MBRCA • Can be few months to years (Vogel et al, Cancer, 1992) • 15 - 90+ months • Depends on sites involved and rate of tumor progression • Volume of disease • Nonvisceral vs visceral • Receptor status (?HER2) • Response to Rx Yamamoto et al, JCO, 1998
MEDIAN OVERALL SURVIVAL ~ 2 years (26 months, Vogel JCO, 1992) NCDB, Five Year Survival Table for Cases Diagnosed in 1998 and 1999
CLINICAL VIGNETTE • 64 yo F presents with new dry cough, progressive over last several weeks • Stage IIB infiltrating ductal, HR+,HER2- diagnosed in 2002 • S/p lumpectomy, AC x4, XRT and 5 yrs of AI • 40 pack-yr history • Work up reveals….
SUSPECTED RECURRENCE…. • Establish diagnosis • ? Need to biopsy • 13-40% discordance in receptor status between primary tumor and metastasis • Restage • CBC, LFTs, imaging
DIAGNOSIS ESTABLISHED…. • Estimate prognosis • Burden and location of mets • Estimate likelihood of response to Rx • Disease free interval • Tumor factors • Establish goals of therapy
CURRENT TREATMENT PHILOSOPHY • MACROmetastasis = expression of systemic disease • Locoregional therapy • Appropriate if impending local complication • Palliative benefit • Generally, no improvement in survival Systemic medical therapy backbone of Rx
GOALS OF SYSTEMIC THERAPY Controlling disease • Palliation • Prolong survival ==> no prospective randomized clinical trials showing therapy extends survival over BSC “Cure” Greenberg et al, JCO, 1996 • 1581 pts with met BrCa • CR with therapy = 16% • Alive and still in CR at 5 yrs = 1.6%
“TREATABLE BUT NOT CURABLE” • Prolong survival with as few symptoms and side effects as possible…. • Data where available, often no head-to-head trials of the multiple therapies…. • OS remains gold standard
SYSTEMIC THERAPIES • Bisphosphonates • Endocrine therapies • HER2 targeted therapies • Conventional chemotherapy (cytotoxics) • Other biologics Toxicity
BISPHOSPHONATES • Reduction of bony complications (Thierhault et al, JCO, 1999) • Which agent? Zolendronate, pamidronate • When to start? 1st met, 1st bony met…. • Timing? q4wks, q3mos…. • When to stop??
PREDICTIVE FACTORS, RESPONSE TO HORMONAL THERAPY (TAMOXIFEN, ARIMIDEX) • McGuire et al, BCRT, 1987
AGENTS • Ovarian ablation/suppression • Hormone withdrawal • SERMs • Tamoxifen • Toremifene • Aromatase inhibitors • Steroidal: exemestane • Non-steroidals: anastrozole, letrozole • Estrogen receptor down-regulators • Androgens/estrogens/progestins • Megesterol acetate
ENDOCRINE THERAPY • Which patients? Low risk pt (HR-?) • How likely to respond? • 10-40% RR, SD 20-30% • For how long? • Response duration variable • When to use? Used early: low toxicity, good chance of response Wilcken N, Hornbuckle J, Ghersi D. Cochrane Database of Systematic Reviews 2003
ENDOCRINE THERAPY • What to use? • PRE: Tam vs ovarian suppression vs ??? • POST: AI > Tam for RR, OS, TTP (11% benefit in relative HR, Mauri, JCNI, 2006) • 2nd line: evidence for tam, fulvestrant, another AI • 3rd, 4th….. ??? • Combinations? • ET combos: tam+ovarian ablation, no study for AI + Tam in metastatic disease • ET + cytotoxics: likely no survival benefit(Fossati et al, JCO, 1998 )
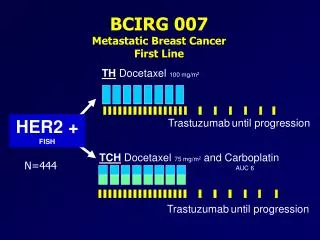
HR+ AND HER2+ • Conflicting evidence….. • TanDem Study • Median OS 28.5 months A+H 25.1 months A-->H 17.2 months A alone Clemens et al, ASCO Breast 2007, #231
PREDICTIVE FACTORS Vogel et al, JCO, 2002
HER2 TARGETED AGENTS • Trastuzumab (humanized, monoclonal Ab) • Lapatinib (small molecule, tyrosine kinase inhibitor [TKI] of EGFR and HER2) • Pertuzumab (monoclonal Ab, blocks dimerization of HER2/3) • CI-1033, pan-HER TKI
TRASTUZUMAB • Can use with or without chemo • Monotherapy: RR close to 30%, clinical benefit rate close to 50% (Vogel et al, JCO, 2002) • Combination: up to 63% RR, TTP 9 mos for docetaxel + tras, minimal add’l toxicity (Esteva et al, JCO, 2002) • When to stop? Slamon et al, NEJM, 2001
LAPATINIB • Capecitabine/lapatinib vs monotherapy • RR 22% vs 14%, p = 0.09 • TTP 8.4 vs 4.3 mos, p <0.0001 • OS not sig • Pts progressing on trastuzumab combined with capecitabine • Other combinations? • Monotherapy 1st line: RR 24%, TTF 16.1 wks (Gomez et al, JCO, 2007) Geyer et al, NEJM, 2006
ESTABLISHED AGENTS • Anthracyclines (doxorubicin, mitoxantrone, liposomal doxorubicin) • Anti-mitotics (taxanes, vinorelbine, ixabepilone) • Anti-metabolites (5FU, capecitabine, methotrexate) • Alkylators (cis/carboplatin) • Gemcitabine • Etoposide
CHEMOTHERAPY • Which patients? • When? Consider if (NCCN consensus-based): • Visceral disease with symptoms • Patients failing ET • Hormone receptor negative • Rapidly progressing?
SINGLE AGENTS • What to use first? No studies to suggest optimal sequence • What dose? No advantage to higher dose • Schedule? Weekly vs q3Wks, esp for taxanes (CALGB 9840) • How likely to respond? First line, RR 30-50% • Continuous vs intermittent? PFS prolonged, but probably not OS (Muss et al, NEJM 1991)
E2100 • Paclitaxel/bev vs paclitaxel wkly (first-line) • PFS 11.8 vs 5.9 mos • OS 26.7 vs 25.2 mos (NS) • RR 36% vs 21% • Grade 3+ CVAs 1.9% Miller et al, NEJM 2007
BEVACIZUMAB • AVADO study (ASCO 2008) • Doce/bev 15 or 7.5 vs docetaxel q3wk alone • RR 63.1% vs 55.2% vs 44.4% • PFS: 8.8 vs 8.7 vs 8.0 mos • HER2+ patients? (phase II, Pegram SABCS 2006) • Dose? • When to stop? • 2nd line? (Miller et al, JCO, 2005) • Combinations? (Xcalibur trial, RIBBON-1 and 2)
SUMMARY • Choose therapy MOST likely to work with LEAST toxicity • Monitor pt for response and toxicity • When to stop actively treating the cancer in mBrCa??? • Return to our patient: • Visceral mets • Symptomatic • ER+PR+ HER2- What’s the right therapy choice?