Download
1 / 29
360 likes | 1.22k Views
Fall 2009 By: Rashidat Akinsanya , RN, BSN, Laura Dawson, RN, BSN, Jennifer Helzer , RN, BSN, Ruslan Moncada , RN, BSN, & Tania Randell , RN, BSN Philosophical Theoretical and Ethical Basis of Advanced Practice Nursing, Johns Hopkins School of Nursing, Baltimore, Maryland.

E N D
Fall 2009 By: RashidatAkinsanya, RN, BSN, Laura Dawson, RN, BSN, Jennifer Helzer, RN, BSN, RuslanMoncada, RN, BSN, & Tania Randell, RN, BSN Philosophical Theoretical and Ethical Basis of Advanced Practice Nursing, Johns Hopkins School of Nursing, Baltimore, Maryland Patient Safety in the ICU! Utilizing the Neuman Systems Model To prevent Catheter Related Blood Stream Infections one patient at a time…
Problem: Catheter Related Blood Stream Infections (CRBSI’s) in the ICU • Magnitude of problem: • CRBSI’s is a large problem, mostly seen in hospitals critical care units, which increases the patients mortality and morbidity rates. • According to the World Health Organization, nosocomial infections are the major cause of morbidity and mortality and it’s also evidence of poor quality of health. (Dulcel, 2002) • Furthermore, this problem is preventable. Institutions can save up to $588,302 per year just by preventing 13 CRBSI’s per year. (Quality and Safety Research Group, JHU, 2008)
Problem: CRBSI’s in the ICU STATS • There is an estimated 250,000 cases of CRBSI’s in hospitals in the US, 80,000 are in ICU’s (CDC, 2005). • There are up to 28,000 deaths in the US per year related to CRBSI’s, attributable mortality is estimated at 12%-15% for each infection (Pronovost et al., 2006 & CDC 2005). • They cost 2.3 billion annually, average cost per patient with a CRBSI is $45,000 (Pronovost et al., 2006). • 10%-30% of nosocomial infections involve the bloodstream (Begany, 2000).
Relevance to Nursing • Nursing is in a perfect position to prevent CRBSI’s… • Nurses are at the forefront of patient safety in hospitals. Nurses serve as patient advocates and must ensure patient safety including the ability to implement measures to control the spread of nosocomial infections.
Relevance to Nursing • In fact, we have an ethical responsibility to do no harm, and in turn we must do everything in our power to prevent CRBSI’s. Our patients put their trust in us to protect them. Having better control over poor technique when inserting central line catheters protects the patients from needless infections. Our ICU patients are already weak and compromised. To allow for possible introduction of pathogens would be irresponsible on the part of nursing.
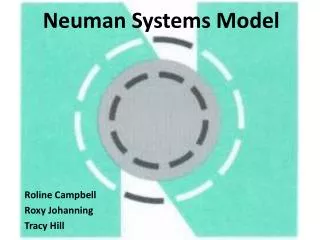
Neuman Systems Model • Wellness oriented and holistic & is based on concepts of stress and reaction to stress. • The Client system consists of 5 interacting variables, which are in constant dynamic interaction: • Physiological – bodily structure and internal function • Psychological – mental processes & interactive environmental effects • Sociocultural– combined effects of social-cultural conditions & influences • Developmental – age-related development processes • Spiritual – spiritual beliefs and influences (Fresse, 2006)
Neuman Systems Model • Draws from the Gesalt theory – homeostasis is the process by which an organism maintains its equilibrium, and thus its health. Many needs exist and each may disrupt a clients balance or stability. • When the stabilizing process fails, or when the client remains in a state of disharmony for too long and is consequently unable to satisfy its needs, illness may develop. (Fresse, 2006)
Neuman Systems Model • Basic Client Structure – Client as a system is composed of a central core surrounded by concentric rings. The inner circle represents the basic survival factors or energy resources such as innate or genetic features. • Lines of Resistance (LOR)– Series of broken rings surrounding the basic core structure, which represents resource factors that help the client defend against a stressor such as the body’s immune response system. • Normal Line of Defense (NLD) – The model’s outer solid circle, which represents a stability state for the individual or system. It includes system variables and behaviors such as the individual’s usual coping patterns, lifestyle, & developmental stage. • Flexible Line of Defense (FLD)– The model’s outer broken ring perceived as a preventive buffer for preventing stressors from breaking through the NLD. The client’s 1st protective mechanism. (Fresse, 2006)
Neuman’s Systems Model • Concepts of levels of prevention • Primary Prevention – Involves reducing the possibility of encountering the stressor or strengthening the client’s normal line of defense to decrease the reaction to the stressor. • Secondary Prevention – Attempts to reduce the effect or possible effect of stressors through early diagnosis & effective treatment of illness symptoms. Strengthening the internal lines of resistance. • Tertiary Prevention – Attempts to reduce the residual stressor effects & return the client to wellness after treatment. (Fresse, 2006)
Evaluation of Theory • Significance The Neuman Systems Model does have significance. It is constructed in a way that is applicable in the real world of nursing. Neuman even offers an integrative review of the model in practice, research, education, and administration. The Neuman Systems Model gives an opportunity for nurses to address essential issues by making them aware of different levels of patient stress, areas for intervention, and by providing a practical assessment and intervention tool.
Evaluation of Theory • Consistency Neuman Systems Model does show consistency. It repeatedly focuses on a holistic approach, the wellness continuum, effects on the patient from the environment, and opportunities for prevention by nursing. Neuman’s Model reinforces its concepts and theoretical assertions throughout explanation of the theory. • Clarity What makes the Neuman Systems Model easiest to understand is the diagram that she created to demonstrate her points of view. It clearly presents her concepts of the layers of stressors on patients, the wellness continuum, and opportunities for nursing prevention and intervention.
Evaluation of Theory • Adequacy The model is a framework utilized in health care that allows for collaboration with all members of the health care team in prevention practices enforcing a holistic approach in caring for the patients. This model is adequate because it provides a framework to be used among health care workers to establish interventions in prevention of CRBSI’s. • Feasibility The Systems Model has proven to be feasible. The model is used extensively in several different countries. It is one of the three most frequently used conceptual models of nursing for research. (Neuman, 1996)
Rationale • Neuman’s System Model is an effective choice of theory related to CRBSI’s since it discusses interference with the body’s Flexible Line of Defense (FLD) as well as prevention of infection. • For example, “the skin is a protective barrier that acts as the flexible line of defense.” Central line insertion breaks down this FLD, exposing the NLD. • Without proper central line insertion technique as well as maintenance, the patient is predisposed to unnecessary central line infections. (Freiberger, 1992)
The Solution Ensure Patients Reliably Receive Evidence Pronovost: Health Services, Research, 2006
The SolutionIdeas for ensuring patients receive the interventions... • Engage: stories, show baseline data • Educate staff on evidence • Execute • Standardize: Create line cart • Create independent checks: Create BSI checklist • Empower nurses to stop takeoff • Learn from mistakes: review infections • Evaluate • Feedback performance • View infections as defects
The Solution Preventing blood CRBSI’s at JHH by utilizing: • The line cart a complete and mobile catheter insertion cart. Keeping all necessary equipment for line insertion so accessible helps the staff maintain strict sterile technique. • VAD Policy – Clear protocol on Central Line maintenance. • The central line insertion checklist – & Empowering the frontline providers empowers nurses to stop line insertion /rewire if provider is not following proper protocol. As of January 2006, all patient care units at JHH have adopted the checklist. Other hospitals across the U.S. have also adopted the guidelines.
CRBSI Rate in Johns Hopkins Hospital’s Adult ICU’s2001- June 2008
The Solution • Very cost effective solution that we would like to see expanded to all critical care units throughout the world.
Problems that might occur? • Fear of change by the organization. The fear of failure in implementing the intervention. Failing might also bring about financial constraints. The organization must have the means to provide adequate resources to implement the intervention. • lack of communication from organization to staff leading to knowledge deficit. There could be lack of communication occurring between the institution’s administration and the staff. The doctors and nurses must be well educated about the importance of this intervention and how its relevance in better patient outcomes prior to implementation.
Problems that might occur? • The staff are not fully committed- lack of buy-in from staff could lead to resistance. The health care team may view this as just another checklist that must be completed and not really take it seriously. They may not view CRBSI’s as a serious problem and need more education. • Physicians- May feel that they don’t have time for these detailed steps or that their care is being scrutinized by those completing the checklist. • Nurses- May also feel that they don’t have time, feel resentful about “policing” physicians or feel that they look like the bad guy if all nurses don’t participate.
Problems that might occur? • Emergency situations • what is an emergency situation? It may become difficult to determine the situations where it is ok to opt out of the behavior change, for example- Is a “code” a good time to follow sterile procedures? And who defines the risk vs. benefit of slowing down line placement for proper technique vs. placing the line as quickly as possible? • Line placed emergently must be rewired within 24hr’s. • Lack of Maintenance of CRBSI Intervention • Someone will need to take responsibility for equipment, paperwork, collection of data, and communication back to staff. Without a champion on each unit, it is likely that this procedure will not be followed and followed correctly.
Bet With Betty Ready to Play?.....
References Begany, T. (2000). Can we do more to prevent nosocomial bloodstream infections? Pulmonary reviews.com. Trends in pulmonary and critical care medicine, 5(7). Retrieved from http://www.pulmonaryreviews.com/jul00/pr_jul00_bloodinfections.html Dulcel, G., Fabry, J., & Nicolle, L. E. (2002). Prevention of hospital-acquired infections: A practical guide. Geneva: World health organization. Retrieved from http://www.who.int/csr/resources/publications/drugresist/whocdscsreph200212.pdf Freiberger, D. , Bryant, J. , & Marino, B. (1992). The Effects of Different Central Venous Line Dressing Changes on Bacterial Growth in a Pediatric Oncology Population. Journal of Pediatric Oncology Nursing, 9(1), 3-7. doi: 10.1177/104345429200900102 Freese, B.T. (2006). Systems model. In A. M. Tomey & M. R. Alligood (Eds.), Nursing theorists and their work. (pp. 318-354). St. Louis, MO: Mosby-Elsevier
References Pronovost, P. , Needham, D. , & Berenholtz, S. (2006). An Intervention to Decrease Catheter-Related Bloodstream Infections in the ICU. The New England Journal of Medicine, 355(26), 2725-2732. Retrieved from http://content.nejm.org/cgi/content/full/355/26/2725 Neuman, B. (1996). The Neuman Systems Model in Research and Practice. Nursing Science Quarterly, 9(2), 67-70. doi: 10.1177/089431849600900207 Center for Disease Control (CDC) (2005, October 14). Reduction in central line-associated bloodstream infections among patients in intensive care units. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5440a2.htm Johns Hopkins University, Quality and Safety Research Group (2008). On the cusp: Stop BSI, Central line-associated blood stream infection toolkit. Retrieved from http://safercare.s3.amazonaws.com/support_media/docs/clabsi/CLABSI_Toolkit.doc