Clinical Diagnosis and Treatment of Ectodermal Dysplasia
2.28k likes | 2.36k Views
Understand the features, pathophysiology, and oral manifestations of Ectodermal Dysplasia in an 8-year-old patient with hypodontia and conical teeth. Learn about confirmation, treatment, and related disorders.

Clinical Diagnosis and Treatment of Ectodermal Dysplasia
E N D
Presentation Transcript
Skin disorders Maji Jose
Clinical details A 8 year old male patient was brought to your dental clinic with complaints of missing teeth. O/E patient has severe hypodontia with the teeth present are conical in shape 1. What is your clinical diagnosis ? 2. To confirm the diagnosis what other features will you look for? 3. What would be your line of treatment?
Scanty hair Frontal bossae Scanty eyebrows Depressed nasal bridge Conical teeth
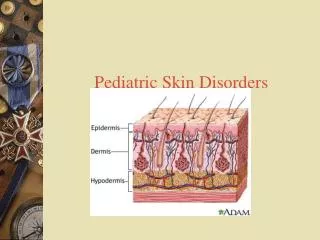
The ectodermal dysplasias (EDs) comprise a large, heterogeneous group of inherited disorders that are defined by primary defects in the development of 2 or more tissues derived from embryonic ectoderm. • The tissues primarily involved are the skin, hair, nails, eccrine glands, and teeth.
Pathophysiology • Ectodermal dysplasia results from the abnormal morphogenesis of cutaneous or oral embryonal ectoderm ( hair, nails, teeth, eccrine glands).
Hair defects: • A reduction in the number of hair follicles in conjunction with structural hair shaft abnormalities may be seen. • Most patients have fine, sparse, lusterless, fair hair resembling lanugo • Scanty / Absence of eyebrows and scalp hair • Beard & mustache are not affected
Exocrine glands defects • Sweat glands may be absent or sparse and rudimentary, particularly in patients with hypohidrotic ectodermal dysplasia leading to Hyperthermia . • Hypoplasia of the salivary and lacrimal glands may occur. In some patients, mucous glands may be absent in the upper respiratory tract and in the bronchi, esophagus, and duodenum. • This may lead to xerostomia, Xerophthalmia (decreased tears) and conjunctivitis and laryngitis and pharyngitis, otitis, and rhinitis
Dental defects • Abnormal morphogenesis ( conical) or complete or partial absence of teeth may occur.
Nail dystrophy: • Abnormal nail plate formation may result in brittle, thin, ridged, or grossly deformed nails.
Other signs and symptoms • short stature and the typical facies, which is often not recognized until infancy, is characterized by frontal bossing; sunken cheeks; saddle nose; thick, everted lips; wrinkled, hyperpigmented periorbital skin; and large, low-set ears • Deficient hearing or vision • Developmental delay or mental retardation
ORAL MANIFESTATIONS • Dental manifestations include conical or pegged teeth, hypodontia or complete anodontia, and delayed eruption of permanent teeth. • Poorly developed alveolar bone leading to decreased vertical height and over closure of mouth and protuberant lips. • Xerostomia (decreased saliva) and frequent dental caries
Important features • Hypohydrosis • Hypotrichosis • hypodontia
Scanty hair Frontal bossae Scanty eyebrows Depressed nasal bridge Conical teeth
Chondroectodermal dysplasia(Ellis-van Creveld syndrome) • Hereditary condition with close resemblance to ectodermal dysplasia • Features are • Ectodermal defects involving teeth, nails • Chondro dysplasia • Polydactyly • Congenital heart disease
Hypoplastic nais with koilonychia • Normal sweating • Short & thick legs and arms • Bilateral polydactyli
O/M • Fusion of middle portion of upper lip to gingiva obliterating the sulcus and causing hypoplasia of upperlip • Natal teeth, premature eruption of deciduous teeth, congenital absence of teeth, irregular spacing, defective shape, enamel hypoplasia,and some times supernumerary tooth
Terminologies • Macule - Flat well circumscribed area of change in normal skin colour. • Patch- Large, flat, non-palpable lesion (>1 cm).
Papule - Solid elevated lesion upto 1 cm in diameter • Plaque - Flat, Solid elevated lesion more than 1 cm in diameter (Formed either by extension or coalescence of papules) • Nodule - Palpable, round or ellipsoidal elevated lesion greater than 1 cm in diameter. (must be palpated to appreciate)
Vesicle - Fluid filled circumscribed elevated lesion upto 1 cm in diameter.They arise from cleavage at various levels of skin. • Bulla - Fluid filled circumscribed elevated lesion greater than 1 cm in diameter • Pustule - Circumscribed elevation of skin that contains a collection of pus.
Common Primary Lesions • Profile <1 cm >1cm Flat Macule Patch Elevated Papule Plaque Palpable(Deep) Nodule Tumor Fluid filled Vesicle Bulla
Crust - Develops when serum, blood, purulent exudate dries on the skin surface • Scale - Cornified cells that become visible on the skin surface. E.g. Psoriasis • Ulcer - It is a break in the continuity of covering epithelium – skin or mucous membrane • Erosion - Shallow defect in the mucosa which involves loss of epithelium but not including basal cell layer.
Fissure - Linear defect that extends from skin surface into dermis. • Dyskeratosis - Disturbance in normal keratinisation resulting in premature keratinisation
Vesiculobullous Diseases Infectious (viral) Non-infectious (mucocutaneous)
Vesiculobullous diseases: infectious • Herpes Simplex (HHV I [(II]) • Primary • Recurrent • Varicella-zoster (HHV III) • Primary • Recurrent • Coxsackie • Herpangina • Hand-foot-mouth disease • Lymphonodular pharyngitis
Vesiculobullous diseases: non-infectious • Immune-related • lichen planus (Bullous) • Erythema multiforme • Stevens-Johnson syndrome • Toxic epidermal necrolysis • Autoimmune • Pemphigus vulgaris • Cicatricial pemphigoid • Bullous pemphigoid • Dermatitis herpetiformis
Non-immunologic / Genetic • Epidermolysis bullosa • Darier-White disease (keratosis follicularis) • Benign familial pemphigus • Miscellaneous • “Allergic” stomatitis • Stomatitis venenata • Stomatitis medicamentosa • Metal & food allergy
Erythema multiforme is a type of acute but self limiting dermatitis, possibly mediated by deposition of immune complex ( mostly IgM ) in the superficial microvasculature of the skin and oral mucous membrane • It usually follows an antecedent infection or drug exposure. • Multi forme – multiple forms
Types • E. multiforme minor - mild, self-limiting • E. multiforme major - severe, life-threatening form • Steven – Johnson Syndrome • Toxic epidermal necrolysis
Causes • Cause is unknown • Erythema multiforme is a type of Hypersensitivity / allergic reaction that occurs in response to medications, infections, or illness. • Medications include: • Barbiturates • Penicillins • Phenytoin • Sulfonamides • Infections include: • Herpes simplex • Mycoplasma • Histoplasmosis
vaccination • Malignancy • Hormonal • Collagen vascular disease • Immunologic disorders • Physical/mechanical factors (tattooing, radiotherapy, cold, sunlight)
Approximately 50% of cases are idiopathic, with no precipitating factor identified. • Emotional factors / stress may be playing a role.
EM minor - Typical targets or raised, edematous papules distributed acrally • EM major - Typical targets or raised, edematous papules distributed acrally with involvement of one or more mucous membranes; epidermal detachment involves less than 10% of total body surface area (TBSA). • SJS/TEN - Widespread blisters predominant on the trunk and face, presenting with erythematous or pruritic macules and one or more mucous membrane erosions; epidermal detachment is less than 10% TBSA for SJS and 30% or more for TEN.
Clinical features • Age – any age , usually children &young adults • Gender – Males are more affected • Seasonal - spring
Erythema multiforme • Nonspecific prodromal symptoms including fever, malaise, myalgias, arthralgias, headache, sore throat, cough, nausea, vomiting, and diarrhea • Sudden onset of rapidly progressive, symmetrical, and cutaneous and/or mucocutaneous lesions (Erythematous macule, papule, Pathches, vesicle or bullae) destributed in a symmetric manner on face ,neck, extremities. • Centripetal spread • Burning sensation in affected areas • Pruritus generally absent • Postinflammatory hyperpigmentation or hypopigmentation may occur.
Classic Presentation • "TARGET LESION" OR “BULL’S EYE LESIONS” • Center Bulla or pale area representing resolution with concentric erythematous rings of varying shades, separated by skin of relatively normal color. • Located on the upper body, legs, arms, palms, hands, or feet