Download
1 / 14
1.06k likes | 6.5k Views
Polycythemia of the Newborn. Lynsey Zuar, D.O. September 2013. Definition of Polycythemia. An increase in the number of erythrocytes in the blood that may be primary or secondary to other causes Hct > 65% on peripheral venous blood draw Hg > 22 g/dL. Normal H&H values in Newborn.

E N D
Polycythemia of the Newborn Lynsey Zuar, D.O. September 2013
Definition of Polycythemia • An increase in the number of erythrocytes in the blood that may be primary or secondary to other causes • Hct > 65% on peripheral venous blood draw • Hg > 22 g/dL
Normal H&H values in Newborn • 26-30wk GA: • Hb: 13.4 • Hct: 41.5 • 28wk GA: • Hb: 14.5 • Hct: 45 • 32wk GA: • Hb: 15.0 • Hct: 47 • Term: • Hb: 16.5 • Hct: 51 • 1-3day: • Hb: 18.5 • Hct: 56
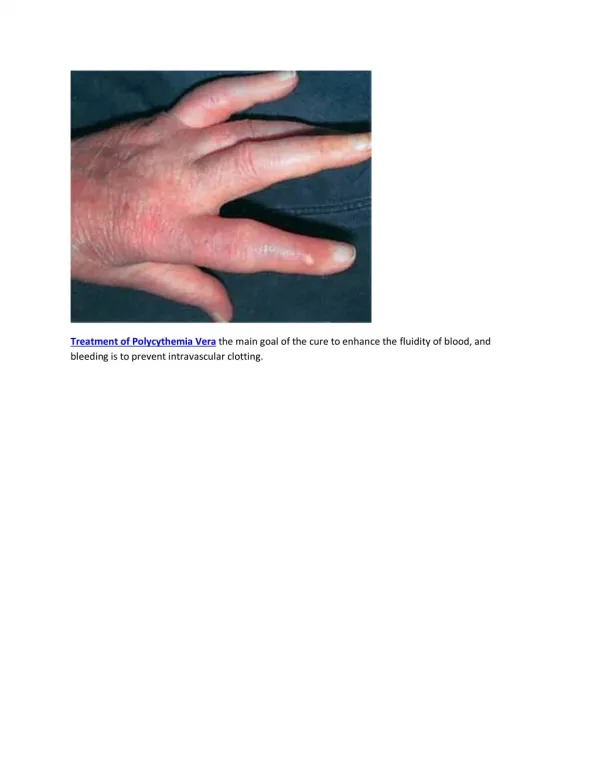
Plethora of a Newborn [pic] • A newborn with high Hct will have a “ruddy” complexion • Dark reddish to purple
Risks of Polycythemia • Increased blood viscosity can be seen with a Hct over 65% • This increased viscosity can lead to end organ damage with microthrombi • The most vulnerable organs are the: • Brain • Kidneys • Adrenal Glands • Can also see hypoglycemia & hyperbilirubinemia in newborns with high Hct from increased erythrocyte destruction and metabolic demand of extra cells. • Should also check POC and TBili
Causes of Polycythemia • Transfusion • Delayed cord clamping/Holding baby below introitus at delivery • Twin-to-Twin transfusion • Maternal-to-Baby transfusion • Hypoxia in utero • Maternal smoking • Placental insufficiency during pregnancy • PIH • Mother’s with cyanotic conditions – aka congenital heart dz • Post-dates newborn • Maternal Diabetes (DMI/DMII/GestDM) • Fetal/Congenital Causes • Trisomy 21, 18, 13 • CAH • Beckwith-Wiedemann Syndrome • Congenital hypothyroidism – check TSH
Who to Screen • IUGR babies • LGA babies • Babies of Diabetic mothers • Trisomies 18, 13, 21 • The bigger of discordant twins • Babies with delayed clamping of umbilical cord • Babies found to have hypothyroidism
How to Screen • Initially you can screen with a capillary heel stick • If Hct >65% then you must confirm with a peripheral venous blood draw • In a newborn found to have borderline high Hct you should rescreen at 6H of life • If it is >65% consider transfer to the NICU for hydration therapy or other therapies • If borderline still – rescreen at 12H of life and treat if >65% • Most newborn’s with high Hct 2/2 cord clamping should have their Hct drop back down to normal levels around 12H of life.
Early Signs & Symptoms • Poor feeding/suck & vomiting • Jittery/Irritability • Hypotonia • Ruddy complexion or cyanosis • Tachycardia/Tachypnea • Respiratory distress • Priapism in males • Hypoglycemia symptoms & sequalae • Jaundice
Late Signs & Symptoms - Untreated • NEC • Cardiomegaly • Decreased CO • Oliguria/Anuria/Acute renal failure • Renal vein thrombisos • Stroke – with neurologic sequlae • Necrotic fingers/toes/penis • Adrenal insufficiency • Testicular/ovarian infarcts and subsequent infertility
End organ effects of Microthrombi • Microthrombi can lead to hypoxia, hypoglycemia, and acidosis in the newborn • The most vulnerable organs are the brain, kidneys, and adrenal glands • Can lead to decreased circulation in extremities as well leading to necrosis of finger or toes
Diagnosis Overview • Screen at risk patients with heel stick – clinical assessment and birth history • If heel stick Hct is high get a peripheral venous blood draw • Remember to rule out dehydration • Also check Tbili, Glucose, & TSH if venous blood shows Hct > 65% • Range of the Hct will dictate which treatment to start • If symptomatic (regardless of range) should be transferred to NICU to start partial exchange transfusion
Treatment Overview • If Hct b/t 65-70% • You can start with monitoring baby for signs and symptoms, and get blood draws q6hrs • More conservative treatment calls for IVF hydration with close monitoring of symptoms and Hct • If Hct b/t 70-75% • Hydration with IVF and close monitoring of symptoms and Hct • If Hct > 75% • Partial exchange transfusion • Some articles and studies theorize that exchange transfusion may increase the chance of NEC in these newborns and that statistical numbers of NEC a/w Polycythemia are skewed because of this
References • www.aap.org • www.uptodate.org • The Harriet Lane Handbook nineteenth edition • www.medscape.com • Rudolph’s textbook of Pediatrics