Download
1 / 34
350 likes | 477 Views
Learn to differentiate and manage preseptal and true orbital cellulitis, a serious ocular condition. Find out about causes, clinical presentation, complications, and treatment options.

E N D
Diseases of the orbitOrbital Cellulitis Dr. Ayesha S Abdullah 19.08.2016
Learning objectives By the end of the lecture the students should be able to • Differentiate between preseptal and true orbital cellulitis • Explain why it is considered to be an ocular emergency • Describe the causes, • Explain the clinical presentation, complications & line of management of orbital cellulitis
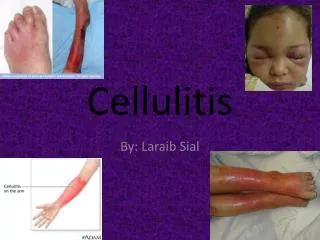
Orbital cellulitis • Preseptal cellulitis • True orbital cellulitis
Preseptal orbital cellulitis • Infection of the subcutaneouss tissue anterior to the orbital septum ( lids) • Causes: • Trauma; lid laceration/ insect bite • Spread from local infection; stye/ dacrocystitis, dental infection • Spread from remote infection; haemotogenous spread from middle ear/ Upper Respiratory Tract
Preseptal orbital cellulitis • Clinical presentation • Symptoms; History of predisposing factor, pain & swelling of the lid, mild fever • Signs; red swollen tender lids sometimes the lids may be difficult to open. Important negative signs are: • Eye itself is normal at the most might be mildly congested • Visual acuity is normal • No proptosis • No ocular motility problem • Normal pupils
Preseptal orbital cellulitis • Complications • True orbital cellulitis • Lid abscess • Cavernous sinus thrombosis
Management of Preseptal orbital cellulitis • Symptomatic; analgesics & NSAIDS • Specific: • Very severe infections may require Adults: 250 – 500 mg oral Co-amoxiclav qds/ tds depending on severity of infection. • Children: 20-40mg/kg/day oral co-amoxiclav over 24h in three divided doses. • benzylpenicillin 2.4-4.8 mg I/M 6 hourly in severe infections • Lid abscesses should be drained • Third generation cephalosporins in penicillin allergy
Orbital cellulitis • Infection of the soft tissues behind the orbital septum ( deeper to lids) • Ocular emergency , could be life threatening • Most frequent pathogens are; • Strept. Pneumoniae , • Staph aureus, • Strept. Pyogenes & H influenzae - (under 5yr)
Causes • Spread from the sinuses; mostly ethmoidal in children & young adults • Extension from preseptal cellulitis • Local spread; dacrocystitis, dental infection, facial infection, infection of the eyeball ( panophthalmitis etc) • Haemotogenous spread • Post- traumatic; accidental/ surgical
Clinical presentation • Symptoms; rapid onset painful swelling of the lids & protrusion of the eye, fever, malaise & visual loss ; history of risk factors • Signs; moderate to severe swelling of the lids, reduced visual acuity, proptosis,red eye with chemosis of the conjunctiva, abnormal & painful EOM & pupillary response
Management • Admit • Symptomatic; antipyretic, NSAIDS • Specific ; hospitalization & antibiotic therapy • Ceftazidime/ Cftriaxone/ Cefuroxime 1 g tds , I/V • Mteronidazole 500mg tds, PO / IV • Vancomycin in case of allergy to the above mentioned • Surgical intervention in case of local abscess or unresponsive cases • Consultation with ENT specialist, neurosurgeon & paediatrician if required
Complications Ocular; corneal damage( exposure),raised IOP, vascular occlusions, optic nerve damage, endophthalmitis Intracranial; meningitis, brain abscess, cavernous sinus thrombosis Orbital abscess
Case #1 A 1 year old child presented to the OPD of department of ophthalmology with the complaint of a swollen right upper lid for the last two days. On examination the lid was red, warm & tender to touch. His visual acuity was normal, the eye had mild conjunctival redness, the pupil was normal and the ocular movements were also normal. Watch the photograph….
Some questions • Is the condition confined to the lids or has it involved the eyeball? • Why do you think so? • What more information would you like to have before making a diagnosis?
Some more information……… • The child had a history of insect bite on the lid two days ago, the swelling increased thereafter. The insect bite mark was visible • There was no history of trauma or symptoms suggestive of sinusitis • His temperature was 99.80 F
Some more questions • What should be the management, keeping in mind the nature of the problem? • Is there any role of health education in this case? Let us see an other case……..
Case #2 • A seven year old child was brought the OPD of the department of ophthalmology with a history of swollen left upper lid for the last 5 days. He also had fever for the last two days. On examination the child had a grossly swollen lid. The doctor had difficulty in opening the lid for examination of the eye. The visual acuity was 6/6 OD & 6/18 OS. The lid was warm and tender. The eye was moderately proptosed with conjunctival chemosis. The pupil was slow to react to light and the ocular movements were painful & limited. The temperature was 1010 F & the child looked generally unwell……..
Some questions…. • Is the condition confined to the lids or has it involved inner orbit? • What more information should we ask for to get an idea about the cause of the problem?
The child had a history of recurrent flu and upper respiratory tract infections. He had history of blocked nose and thick greenish nasal discharge was noted on examination. • The child was put on intravenous antibiotics but didn’t get better • Why?
The antibiotics were changed to intravenous ampicillin/sulbactam and after 5 days were changed to oral amoxicillin/clavulanic acid for a total of 14 days of antibiotics.
Some more questions • What should be the management, keeping in mind the nature of the problem? • What do you think can be done with the abscess? • Is there any role of health education in this case? • ..
Conclusion about the two cases • What is the difference between the two cases? • We consider the second case an ocular emergency, why? • Why did the subperiosteal abscess form in the second case? • What other complications could happen in the second case?
Let us summarize • Preseptal orbital cellulitis & orbital cellulitis are both infections. • It is more common in children • The route of infection could be from the nearby infectious focus like infected sinuses, skin wound or spread of infection via blood • The most common cause especially in children is ethmoidal sinusitis
Both preseptal and orbital cellulitis may have: • Fever • Eyelid swelling • Pain • Red eye • Child is ill-appearing
Orbital cellulitis signifies spread of inflammation to the posterior orbital contents that is the eyeball, extraocular muscles: helpful signs to distinguish it are:- • Proptosis • Decreased visual acuity ( may be normal in the beginning) • Red eye with conjunctival chemosis of moderate to intense congestion • Painful limited eye movements • Afferent pupillary defect
Prior to the availability of antibiotics, patients with orbital cellulitis had a mortality rate of 17%, and 20% of survivors were blind in the affected eye. However, with prompt diagnosis and appropriate use of antibiotics, this rate has been reduced significantly • blindness can still occur in up to 11% of cases. Orbital cellulitis due to methicillin-resistant Staphylococcus aureus can lead to blindness despite antibiotic treatment.