Download
1 / 25
250 likes | 462 Views
Post operative complications Classification Specific to operation General ( Immediate early late). E.G Complication of a Bowel Resection for colon ca. Common clinical presentation Low urine output (oligo-anuria)

E N D
Post operative complications Classification Specific to operation General ( Immediate early late)
Common clinical presentation • Low urine output (oligo-anuria) • Urine output is a reflection of GFR which is a reflection of RBF hence hydration • Surgery produces the stress response. Which leads to decreased urine volume. • Other factors can affect GFR not just RBF
Min. acceptable urine output is 0.5ml/kg • Important to act on urine output to avoid tubular damage and necrosis hence acute renal failure
Patient has oligo-anuria Catheterize ? retention If catheter flush If real oligo - anuria Check for low Assess for signs Cardiac output of hypovolaemia
Treat causes of trial of fluid Challenge Low cardiac output bolus up to 5ml/kg (e.g arrhythmias) Consider icu support if failed consider further challenge monitored by cvp
Advanced therapies • Furosemide • Dopamine water • Renal support – indication k+ urea (to toxic bwels) failure to regulate acid-base
2- Confusion (D.A.M HYPOS) • Drugs - Anaesthetic agents - Analgesics (opiates) - Normal drugs being given - Normal drugs not being given
Acute systemic infection - Wound infection - Anastomotic leak - Chest infection
Metabolic disturbance • Hypokalaemia / hyper • Na+ Na+ • Sugar / sugar • Fluid overload - Alcohol withdrawal
Hypotension - Occult haemorrhage • Inadequate fluid infusion • Low cardiac output (MI arrhythmias, PE)
HYPOXIA • PYREXIA
HYPOXIA • Common especially in thoracic + abdominal surgery cause may be multifactorial • Have a low index of suspicion – mild confusion mild hypotension and slight tachycardia may be the only signs -
Basic physiology. Adequate analgesia, proper patient positioning, humidified oxygen and physiotherapy • Most post-op respiratory problems are not due to classical pneumonia. Provided the collapse and hypoventilation that underlies many problems is treated, any infectious element usually settles spontaneously.
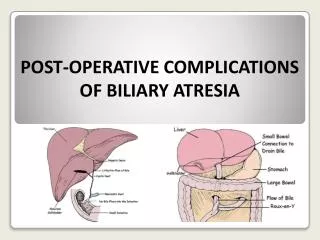
Common or important problems • Anastomotic leak - Between days 4 – 14 postoperatively manefist as • Peritonitis • Intra – abdominal abscess • Enteric fistula. (path or least resistance i.e through wound or drain site)
2- Wound complication • Wound infection • Wound dehiscence. • Wound hernia
3- Cannula related sepsis 4- UTI
5- Intestinal obstruction • Mechanical – uncommon as early complication following surgery – late due to adhesion. • Paralytic
6- Fluid and electrolyte imbalance May occur as a result of. • Inappropriate administration of fluid replacement therapy by the medical staff. • Excessive losses e.g due to NG tubes. High intestinal stoma output , intestinal fistulae, diuretics etc. • Intrinisic renal disease exacerbated by surgery or drugs
7- Thromboembolic disease. • Upto 20% of patients that stay longer than 7 days can develop DVT • Highest in women on ocp + pelvic surgery • Majority will not be clinically apparent .
8- Adhesions • Fibrnonos – usually resolve 6-9 weeks • Can become fibrosed dense fibrotic adhesion. In abdomen these bands of tissue may form between or over loops of small bowel in particular. may lead to “kinking” or compression of small bowel loops, causing obstruction and even infarction of the blood supply. Such complication may occur shortly after the adhesions form. Within months of surgery, or many years after.
Factors that cause adhesion include: • Genetic • Infection/inflammation at time of surgery • Use of powdered (starch) surgical gloves) • Use of biological suture material • Cooling of intestinal loop.