Download
1 / 78
1.06k likes | 1.68k Views
Brain Metastasis: The Role of Radiation. John Crew, M.D. PGY-2, Radiation Oncology. Objectives. Neuroanatomy Epidemiology Clinical presentation of brain metastases Pathologic findings

E N D
Brain Metastasis: The Role of Radiation John Crew, M.D. PGY-2, Radiation Oncology
Objectives • Neuroanatomy • Epidemiology • Clinical presentation of brain metastases • Pathologic findings • Discuss the roles for Surgery, Whole Brain Radiation Therapy (WBRT) and Stereotactic Radiosurgery used as single modalities or in combination • Outcomes including neurocognitive dysfunction
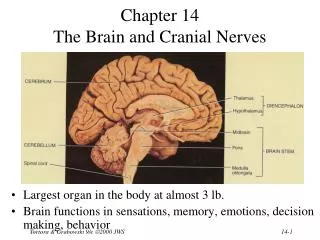
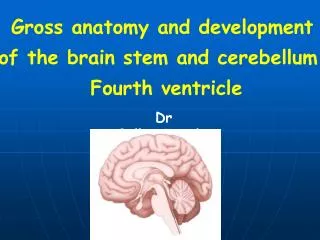
Anatomy Cerebrum Gray-White Junction Cerebellum Brainstem Pons, Medulla Meninges Pia, Arachnoid, Dura “Brain Metastasis” refers to metastatic lesion involving the brain parenchyma (cerebrum, cerebellum, brainstem).
Epidemiology • 170,000 newly diagnosed/year in U.S. • 25% of adult cancer patients • Mean Age: 55-65 years • Increasing Incidence • Aging population • Systemic therapies • Detection
Clinical Presentation Lassman, AB, DeAngelis, LM et al. Brain Metastases. Neurol Clin N Am 2003;21;1-23.
Diagnosis Physical Exam Imaging MRI with Gadolinium T1 post gad Small non-enhancing lesions may be seen on T2 CT Head with contrast – If MRI unavailable May miss small posterior fossa lesions -Lesions enhance as a result of disrupted blood-brain barrier -Can use PET or MR Spectroscopy to consider other etiologies Lassman, AB, DeAngelis, LM et al. Brain Metastases. Neurol Clin N Am 2003;21;1-23.
Histology *Of all cancer types, melanoma is most likely to metastasize to the brain *Hemorrhagic Histologies: Renal Cell Carcinoma, Thyroid, Melanoma
Theories Regarding Metastatic Spread James Ewing (1928) – “Seed and Soil” • Stephen Paget (1889) – Hematogenous spread
Brain mets: Surgical Pathology Sharply demarcated masses Typically at gray matter-white matter junction with zone of edema Boundary between tumor and parenchyma easily seen Often see nodules of tumor with histology consistent with the primary disease
Radiation Modalities • Whole Brain Radiation Therapy (WBRT): Fractionated treatment typically given over 2-3 week time course • Stereotactic Radiosurgery (SRS): Single High-Dose Fraction of Radiation • Linear Accelerator based • Gamma Knife • CyberKnife • Proton
Other Terms • Stereotactic radiotherapy: High dose stereotactically guided radiation given in multiple fractions • Fractionated Stereotactic Radiosurgery: Given in two to five fractions
Whole Brain Radiation Therapy (WBRT) -Treated with two opposed fields using a linear accelerator -Fractionated daily treatments
Linear Accelerator Based Stereotactic Radiosurgery • Single Fraction or Hypofractionated • Frameless or Stereotactic Frame • Photons http://radonc.ucsd.edu
Gamma Knife Radiosurgery • Single Fraction or Hypofractionated • Stereotactic Frame • Cobalt 60 sources
RTOG 79-16 • Phase III • N = 859 • Four arms • 30 Gy/10 +/- misonidazole (1 g/m2) • 30 Gy/5 +/- misonidazole (2 g/m2) • Results • MS 3.9 mo (60% alive at 3 mo, 35% at 6 mo, 15% at 12 mo) • No difference in survival within treatment arms
RTOG 79-16 (cont.) • Subsequent statistical analysis (pre-treatment predictors for 200 day survival) • Favorable -> Age < 60, KPS ≥ 70, controlled primary, brain metastasis only
RTOG 85-28 • Phase I/II – Accelerated Fractionation • Patient characteristics: • KPS > 60 • Controlled or absent primary with either: • Stable extracranial metastatic disease • Only brain metastasis with uncontrolled primary
RTOG 85-28 (cont.) • All patients: • 32 Gy/1.6 Gy bid with boost dose escalated (16 Gy -> 22.4 Gy -> 32 Gy -> 42.40 Gy) • MS: 4.2-6.4 mo increasing with escalating doses • MS also increased in patients with controlled primaries, non-lung primaries, solitary metastasis
RTOG 89-05 • Phase III • WBRT (37.5 GY/15) alone vs. WBRT (37.5 cGy/15) + bromodeoxyuridine • NS between two treatment groups • MS (RT alone) was 6.12 mo vs. 4.3 mo (BrdUrd) • MS increased in patients with solitary brain metastasis.
RPA: Study Design • 1200 evaluable patients (1276 total, 76 excluded) • Prognostic Factors Evaluated • Patient Related: age, KPS, neurologic function, neurologic signs/symptoms • Tumor Related: Primary pathology, status of primary lesion (controlled vs. uncontrolled), presence of extracranial metastasis, # brain mets (single, multiple), time to brain metastasis • Treatment Related: prior surgery to brain, total RT dose, RT response at first follow-up
RPA classes (cont.) MS: 7.1 mo MS: 4.2 mo MS: 2.3 mo 1 2 3
Other Prognostic Scores Neider et al. Prognostic scores in brain metastasis from breast cancer. BMC Cancer 2009, 9:105.
Surgical Management Background (Prior to 1990): Surgery for single brain metastasis controversial. Lack of controlled clinical trials Uncontrolled retrospective trials fraught with conflicting results and selection bias Surgery (prior to 1990) utilized for single brain metastasis occasionally if good prognosis otherwise.
R **All patients received Dexamethasone 4 mg PO q6h from diagnosis to RT completion
Time to recurrence at original site P<0.0001 Surg + RT (n=25) Bx + RT (n=23)
Neurologic Survival P<0.0001 Surg + RT (n=25) Bx + RT (n=23)
Actuarial Survival P<0.01 Surg + RT (n=25) Bx + RT (n=23)
Functional Independence P<0.005 Surg + RT (n=25) Bx + RT (n=23)
Patchell et al. Postoperative Radiotherapy in the Treatment of Single Metastases to the Brain. JAMA 1998, 280:17.
Primary End Point: • Tumor recurrence in the brain • Secondary End Points: • Length of survival • Cause of death • Preservation of functional ability Patchell et al. Postoperative Radiotherapy in the Treatment of Single Metastases to the Brain. JAMA 1998, 280:17.
Recurrence Patchell et al. Postoperative Radiotherapy in the Treatment of Single Metastases to the Brain. JAMA 1998, 280:17.
Patchell et al. Postoperative Radiotherapy in the Treatment of Single Metastases to the Brain. JAMA 1998, 280:17. Time to Brain Recurrence Surgery + WBRT Surgery + WBRT Surgery + WBRT Surgery Surgery Surgery Time to anywhere brain recurrence Time to distant brain recurrence (Anywhere but original site) Time to recurrence at original site of resection
Death due to Neurologic Causes • Death from neurologic causes: • Progressive neurologic dysfunction with stable systemic disease • Severe neurologic disability who died of intercurrent illness • Rapidly progressive systemic disease with declining neurologic function • Death from systemic causes: • Progressive systemic disease in setting of stable or improving neurologic status p < 0.003 Total Deaths: 82 Patchell et al. Postoperative Radiotherapy in the Treatment of Single Metastases to the Brain. JAMA 1998, 280:17.
Death due to Systemic Cause P < 0.01 Patchell et al. Postoperative Radiotherapy in the Treatment of Single Metastases to the Brain. JAMA 1998, 280:17.
Functional Status and Survival p = 0.061 p = 0.39 Patchell et al. Postoperative Radiotherapy in the Treatment of Single Metastases to the Brain. JAMA 1998, 280:17.
WBRT • Response: Histology • Fractionation
Histology and Whole Brain Radiation Nieder et al. Tumor Related Prognostic Factors for Remission of Brain Metastases After Radiotherapy. Int J Radiat Oncol Biol Phys. 1997; 39:25-30.
Histology and Whole Brain Radiation • Sundstrom et al. (Ann Med. 1998 Jun;30(3):296-9) • Retrospective, 75 pts
Whole Brain Fractionation Platta et al. Current Treatment Strategies for Brain Metastasis and Complications from Therapeutic Techniques. Am J Clin Oncol 2009; [Epub ahead of print].
“If WBRT is used, is there an optimal dosing/fractionation schedule?” • Reviewed 18 trials comparing WBRT dosing • Conclusions • Altered fractionation schedules do not result in significant differences in: • Median survival • Local control • Neurocognitive functioning