Download

1 / 13
140 likes | 422 Views
Community Health Partnerships. Angela Canning. What we do. Community Health Partnerships. T o examine whether CHPs are achieving what they were set up to deliver, including : their governance and accountability arrangements how well they are using resources. Audit of CHPs – our methodology.

E N D
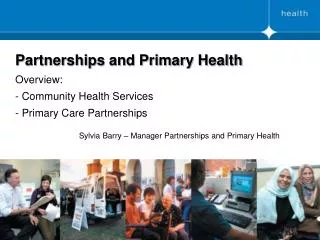
Community Health Partnerships Angela Canning
What we do Community Health Partnerships
Community Health Partnerships Community Health Partnerships • To examine whether CHPs are achieving what they were set up to deliver, including: • their governance and accountability arrangements • how well they are using resources
Audit of CHPs – our methodology Community Health Partnerships • Analysis of published national statistics • Analysis of CHP information held by ISD Scotland • Collected information directly from CHPs (eg structures, budgets, staffing) • More detailed work in 6 CHPs about specific issues • Desk-based review of documentation • Interviews
Main findings (1) – Partnership working in the public sector Community Health Partnerships • Long history to partnership working in the public sector • Cluttered landscape: • Risk of duplication between groups • Lack of clarity on distinct roles and responsibilities • Opportunities to streamline and achieve efficiencies
Main findings (2) – CHP structures Community Health Partnerships • Two types of CHP structure (health-only CHP and integrated CHP) but no evidence that one structure is better than the other • Partnership working is challenging and requires: • clarity of purpose • strong, shared leadership • commitment • good relationships
Good governance principles for partnership working Community Health Partnerships
Main findings (3) – Governance arrangements in CHPs Community Health Partnerships • Governance arrangements are complex and not always clear: • CHPs set up over 5 years ago and have evolved over time • Schemes of establishment (SoEs) are out-of-date or incomplete • Other governance documents are inconsistent with SoEs • Lack of clarity about CHPs’ devolved functions and other responsibilities • Added complexity for integrated partnerships • Lack of clear, joint vision and strategies for health and social care • Performance arrangements are complex and not always aligned with strategies • Joint workforce planning and management arrangements for joint posts are underdeveloped
Main findings (4) – Use of resources Community Health Partnerships • Few CHPs influence how resources are used across the whole system • Joint planning and resourcing is generally underdeveloped: • Need better information about how resources are used • Pooled budgets are beneficial but only one in Scotland • Need better engagement with GPs and other clinicians • SG is leading Integrated Resource Framework project and Change Fund • £13 billion spent on health and social work services in 2009/10: • CHPs managed about £3.2 billion but responsibilities vary • Management and administration costs are unclear • Gaps in community-based activity and workforce information at a CHP level
Main findings (5) – Impact on health and quality of life of local people Community Health Partnerships • Scotland has long-standing health issues • Difficult to attribute change in people’s health to any single body • No large scale shift in the balance of care • CHPs have contributed to some improvements, eg support for rehabilitation, anticipatory care, training for carers, self-management
Current work programme Community Health Partnerships
Future work programme Community Health Partnerships
More information Community Health Partnerships www.audit-scotland.gov.uk acanning@audit-scotland.gov.uk