Download

1 / 24
240 likes | 595 Views
HIV in India. Pauline Harvey, PhD, MSPH American Embassy School January 22, 2011. Outline. Epidemiology Definition Scope of work HIV HIV and AIDS Natural history HIV in India Epidemic Response National AIDS Control Programme Phase III (NACP-III) Websites for more info on HIV/AIDS.

E N D
HIV in India Pauline Harvey, PhD, MSPH American Embassy School January 22, 2011
Outline • Epidemiology • Definition • Scope of work • HIV • HIV and AIDS • Natural history • HIV in India • Epidemic • Response • National AIDS Control Programme Phase III (NACP-III) • Websites for more info on HIV/AIDS
Epidemiology • Definition • Study of diseases in man • Population based • Scope of work • Disease prevention and control programs • Vaccination programs, Outbreak investigation, Emergency response • Strategic Information • Monitoring and evaluation, Surveillance, Operational Research • Capacity building and training • Infectious diseases, chronic diseases, injury prevention, emerging threats, water & food borne illnesses
Epidemiology and HIV Terminology • Prevalence and incidence • Prevalence • Number of cases of a disease in a population • Incidence • Number of new cases of a disease in a population • Rare disease, general and concentrated epidemic • Rare disease • Prevalence less than 0.5% of the population • Generalized HIV epidemic • Prevalence is greater than 1% in Antenatal Clinics • Concentrated HIV epidemic • Prevalence is less than 1% in Antenatal Clinics but greater than 5% among Most at Risk Populations (MARPs)
HIV • What is HIV? • Human Immunodeficiency (suppressive) Virus • Virus discovered in 1983 • Blood test became available in 1985 • What is AIDS? • Acquired Immunodeficiency Syndrome • First reported in 1980 and designated in 1981 (cases of pneumocystiscarinii pneumonia and Kaposi’s sarcoma in LA and New York) • What is the difference? • How does it affect disease control?
HIV • Natural History • Virus • Reduces the effectiveness of the immune system • Symptoms • Opportunistic infections and tumors • Latency • Progressive • Transmission – through bodily fluids • Blood • Semen • Vaginal fluid • Preseminal fluid • Breast milk • What would you do to prevent transmission in a population?
Dynamics of Transmission* MARPs FSW Male Clients MSM IDUs Males Spouses/ Partners Females • General Population • Former MARP • Iatrogenic Children *Adapted from Tim Brown
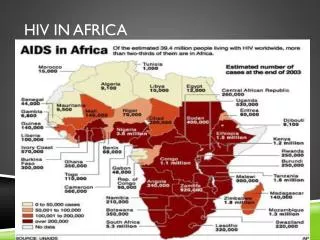
Main Drivers of HIV Epidemic, Globally • Unpaid Heterosexual Intercourse • Between males and females in the general population (African epidemic) • Commercial Sex Work • Between a female or male sex worker and a client (Asian epidemic) • Men who buy sex are the main driving force in Asia and the largest infected population group. • An estimated 10 million Asian women sell sex and at least 75 million men buy it regularly. • Injecting Drug Use • Unprotected anal sex between MSM
HIV Transmission in India • India has the THIRD largest HIV epidemic in the world. • In 2008, the Government of India (GoI) estimated 2.27 million people were living with HIV/AIDS in India. • 3.5% of these were children (79,450) (Over 3 million children AFFECTED by AIDS) • Most at Risk Groups (MARPS) include: • Injecting Drug Users (IDUs) • Men who have sex with men (MSM) • Female Sex Workers (FSWs) • Other risk groups include: • Migrants • MARPs following trucking and trade routes
Some facts on HIV prevalence in India • The estimated Adult HIV prevalence is 0.29% of the Indian population. • 9.2% of IDUs • 7.3% of MSM • 4.9% of FSWs • Prevalence declined from 0.36 % in 2006. • 86% of HIV cases are attributed to heterosexual transmission.
Modes of HIV Transmission, India Not Specified 4.7% MSM 1.4 % Infected Syringe & Needles 1.3% Unprotected heterosexual contact is the main route accounting for 85.6% of the total HIV transmission
HIV and FSWs • FSW • HIV Prevalence ranges from 5% to 40% • 0.5% of adult female population but 7% of HIV infected females • Only 38% ever had an HIV test • Average 10 clients per week • 50% reported at least one Sexually Transmitted Infection symptom • 69% of FSWs were ever married • 46% did not use condom during last sex with non-paying client • Male Clients • 5% of sexually active urban males and 3% of sexually active rural males visited a Sex Worker in the last 12 months. • 75% are in age group 20-35 years • 24 % had sex with more than three FSWs • 64% of clients of Female Sex Workers are ever married • only 13% use condom with their spouse
HIV and MSM • MSM • 3% of adult males reported ever indulged in MSM activities • 10-30% had first sex with male partner before the age of 15 years • More than 50% of MSM are married and have female sexual partners • 30-50% of MSM reported any one STI symptom in last 12 months • 50-60% reported commercial male partners and more than 80% reported non-commercial male partners one month • Average 2-12 commercial male partners in a week • 15% of MSM are at high risk for acquiring/transmitting HIV
HIV in India • Type of epidemic • General or concentrated? • Why be concerned? • Primary mode of transmission • Commercial sex work • How would you control the epidemic?
HIV in India • How would you try to control the epidemic?? • Goal? • What do you want to accomplish? • What is success? • Focus? • Limited resources and competing priorities • MARPs or general population • Resources? • Own resources or donor resources • Three Ones (action framework, national coordinating authority, monitoring & evaluation system) • Other benefits • Spillover
HIV in India • National AIDS Control Organisation (NACO) • National AIDS Control Programme Phase III (NACP III) http://www.nacoonline.org/NACO
NACP-III (2007 – 2012) • Overall goal • Halt and reverse the epidemic in India over 5 years (2007-2012) by integrating programs for prevention, care, support and treatment. • Strategy: • Prevention of new infections in high risk groups and general population through: • Saturation of coverage of high risk groups with targeted interventions (TIs) • Scaled up interventions in the general population • Providing greater care, support and treatment to larger number of People Living with HIV/AIDS (PLHA). • Strengthening the infrastructure, systems and human resources in prevention, care, support and treatment programs at the district, state and national level. • Strengthening the nationwide Strategic Information Management System. • Specific objective • Reduce new infection as estimated in the first year of the program by: • 60% in high prevalence states so as to obtain the reversal of the epidemic; and • 40% in the vulnerable states so as to stabilize the epidemic.
NACP-III (2007 – 2012) • Programme Priorities and Thrust Areas • Learn from the lessons of the previous two phases of NACP • Prioritize preventive efforts • More than 99% of the population is free from infection • Integrate prevention with care, support and treatment. • MARPs will receive the highest priority (Sex workers, MSM, IDU) • Lower priority groups with high levels of exposure (long distance truckers, prisoners, migrants, refugees and street children). • Next priority general population services – STI treatment, voluntary counseling and testing and condoms.
NACP-III (2007 – 2012) • Programme Priorities and Thrust Areas Cont’d • Ensure all persons who need treatment would have access (prophylaxis, opportunistic infections, and first line ARV drugs). • Prevent vertical transmission through universal provision of PPTCT services and assure access to pediatric ART. • Address the needs of children infected and affected by HIV through agencies involved in child protection and welfare. • Invest in community care centers to provide psycho-social support, outreach services, referrals and palliative care. • Work with agencies involved in vulnerability reduction such as women’s groups, youth groups, trade unions etc. to integrate HIV prevention into their activities. • Facilitate a multisectoral response including private sector, civil society organizations, PLHA networks and government departments to provide prevention, care, support, treatment and services.
Other sources of information on HIV/AIDS • US Department of Health and Human Services, Centers for Disease Control and Prevention http://www.cdc.gov/hiv/default.htm • Joint United Nations Programme on HIV/AIDS http://www.unaids.org/en/