Download
1 / 37
370 likes | 383 Views
Learn about different species of atypical mycobacteria, including nontuberculous mycobacteria, laboratory diagnosis, common clinical syndromes, and treatment options.

E N D
Atypical Mycobacterium Ali Somily MD
Nontuberculous Mycobacteria • All mycobacterial species except those that cause tuberculosis (TB) • Mycobacterium tuberculosis complex includes M. tuberculosis • including M. tuberculosis subsp canetti • M.bovis • M. bovis BCG strain • M. africanum • M. caprae • M. microti • M. pinnipedii • Leprosy (M. leprae).
Nontuberculous Mycobacteria • 1954 Runyon first NTM classification • >100 NTM species • Other names • Mycobacteria other than tuberculosis (MOTT) • Atypical • Environmental • Opportunistic • Variable pathogenicity and geographic regions • 40% cause diseases in human • Immunosuppressed host
Nontuberculous Mycobacteria • Water, soil, food and animals • Does not spread from person to another • Relatively resistant to chlorination and ozonization • Outbreak and Pseudo-outbreak in the hospital • HIV and dialysis patients • Improve laboratory methods reporting • MAC 40%,rapidly growing 10%,15% unknown,25% M.gordonae,2.5% M.kansasii(MW USA and UK) and 1% M.xenopi (Ontario)
Laboratory Diagnosis • Rapid Growers • Days in broth and < 1 week in solid media • M.abscessus • M.chelonae • M.fortutum • Slow Growers • 1-2 weeks in broth and 2-4 weeks in solid media • M.avium • M.kansasii • M.scrofulaceum • M.ulcerans • M.xenopi • M.gordonae
Special Diagnostic Problems • M.leprae cannot be cultured • M.marinum lower temperature required • M.haemophilum lower temperature required and iron need to be added • M.ulcerans lower temperature required • M.genavense very slow growth in broth • DNA probes for MAC, M. kansasii and M. gordonae available • Identification and sensitivity
Nontuberculous Mycobacteria • Risk factors • Immunosuppression ( HIV, Medications ) • Aging • BCG vaccination • Cystic fibrosis • Fibronodular bronchiectasis
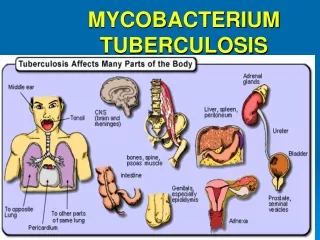
Nontuberculous Mycobacteria • Common clinical syndromes: • Lymphadenopathy • Chronic pulmonary disease • Skin and soft tissue infections (often associated with trauma or a foreign body) sometimes with extension to bone and joint • Disseminated disease.
Nontuberculous Mycobacteria • Pulmonary disease • Definition • Usually adults • Symptoms of cough, sputum production, weight loss • Two or more sputum isolates or one isolate from,BAL,Bx, sterile site • Distribution of isolates varies regionally
Nontuberculous Mycobacteria • Pulmonary disease • Common etiological agents • M. avium complex(MAC) • M. kansasii • M. abscessus • M. xenopi
M.Avium complex (MAC) • Elderly men with COPD • Middle aged to elderly Non- smoking women • CF patients • Hypersensitivity pneumonitis
M.Kansasii • Similar to TB • US midwest and south • AFB positive • Probe positive • HIV CD4 <200 pulmonary and disseminated • M..xenopi • UK, Northern Europe and Canada, less common in US • Rural /farm area • Very good outcome
Nontuberculous Mycobacteria • Pulmonary disease • Treatment • Treatment with combined antimicrobials • Resection if localized
Nontuberculous Mycobacteria • Lymph node disease • Definition • Usually < 5 years of age • Unilateral, submandibular site most common • Onset of symptoms subacute • Skin induration and sinus tract formation may occur • R/O TB • MAC (80%) is the most common followed by M. scrofulaceum • Dx Fine needle or excisional Bx
Nontuberculous Mycobacteria • Lymph node disease • Common etiological agents • MAC • M. kansasii • M. malmoense • M. haemophilum • Uncommon etiological agents • M. scrofulaceum • M.fortuitum/ peregrinum • M.abscessus/ chelonae
Nontuberculous Mycobacteria • Lymph node disease • Treatment • Surgical resection is usually curative
Nontuberculous Mycobacteria • Skin/soft tissue/bone/joint and tendons • Definition • History of trauma or superficial laceration • Presence of a foreign body
Nontuberculous Mycobacteria • Skin/soft tissue/bone/joint and tendons • Common etiological agents • M. marinum • M. fortuitum/peregrinum • M. abscessus/chelonae • M. ulcerans • Uncommon etiological agents • MAC • M. kansasii • M. terrae • M. haemophilum
M.marinum • Water ,fish • Lake, bay,ocean,pool,aquarium • 1-2 month IP granulomatous nodular – ulcerative lesions (hands) • Bx for diagnosis
Buruli ulcer /M.ulcerans • Chronic cutanous ulcer • Africa mostly • Debridment
Nontuberculous Mycobacteria • Skin/soft tissue/bone/joint and tendons • Treatment • Debridement plus combined drug therapy
Nontuberculous Mycobacteria • Disseminated • Definition • HIV or other immunosuppressive disease • Symptoms: fever, weight loss, diarrhea • Any site possible • No trauma necessary
Nontuberculous Mycobacteria • Disseminated • Prevention & treatment • Prevention of MAC in HIV by prophylaxis • Treat positive blood culture aggressively
Nontuberculous Mycobacteria • Disseminated • Common etiological agents • MAC • M. genavense • M. abscessus/chelonae • M. haemophilum • Any mycobacterium may cause disease in association with significant immunosuppression HIV CD4 < 50), and any localized lesion may disseminate.
Rapid Growers • M.fortutum • M.abscessus • M.chelonae • Skin and soft tissue infection after truma , post-op,cardiac ,mammoplasty and cosmotic • Pulmonary M.abscessus>M.fortutum • Indolent, progressive • Cavitary uncommon • Mild systemic symptoms
Leprosy • Worldwide –esp in tropical countries • Transmission rout unknown • Can not be cultured • Syndromes • Lepromatous • Tuberculoid • Mixed • Treatment 6-months to 2 years • Dapsone + Rif +/- clofazimine
Nontuberculous Mycobacterial Disease • Principles of Treatment of NTM Disease • 1. Patients should be carefully evaluated to determine the significance of an NTM isolate. The presence of the organism in a sterile site or repeatedly from airway secretions in association with a compatible clinical and radiologic picture confirms the diagnosis. • 2. Treatment of rapidly growing mycobacteria should be guided by in vitro susceptibilities. Other drug susceptibility testing is not standardized.
Nontuberculous Mycobacterial Disease • 3. Treatment should usually combine at least two drugs of proven efficacy. • 4. Contact follow-up is not necessary since NTM are not transmitted from person to person. • 5. Duration of therapy has not been determined; in general, 6-12 months is required following negative cultures.
Nontuberculous Mycobacterial Disease • 6. In soft tissue infections, because of rapidly growing mycobacteria, a combination of debridement and treatment with antimicrobials is recommended. For selection of antimicrobial agents, consultation with the laboratory should be undertaken regarding the reliability of in vitro testing.
Antimycobacterium • MAC Clarithromycin or azithromycin + ethambutol+Rifampin • M. xenopiRifampin+Ethambiotol +INH • M. kansasiiRifampin + Ethambutol • M. malmoenseRifampin or Ethambutol • M. marinumRifampin or Clari + Ethambutol 2-3 months • Rapid growersdoxycycline, amikacin, imipenem, quinolones, sulfonamides, cefoxitin, clarithromycin
Antimycobacterium • M. haemophilumClarithromycin, Rifampin Cipro or Amikacin • M. genavense Clarithromycin, Rifabutin or AmikacinEthambutol • M. ulceransClarithromycin, Rifampin, Ethambutol or PAS ( Paraaminosalicylic acid) • MAC prophylaxisAzithromycin , Clarithromycin or Rifabutin 300 if CD4 <50x 106/L