Download
1 / 63
630 likes | 1.16k Views
Objectives. To review the indications for intubationTo briefly discuss RSITo review the airway assessmentTo discuss difficult airwaysTo review difficult airway algorithmsTo discuss an approach to difficult airwaysCase discussions . Case. 13 yr/o M mountain bikingNeck vs. handlebarsSitting-up

E N D
2. Objectives To review the indications for intubation
To briefly discuss RSI
To review the airway assessment
To discuss difficult airways
To review difficult airway algorithms
To discuss an approach to difficult airways
Case discussions
3. Case 13 yr/o M mountain biking
Neck vs. handlebars
Sitting-up on bike path
Anterior neck swelling
VSS
Mild stridor
What will you do?
4. The 4 Questions Does this patient need intubation now?
Is this a crash situation?
Is this a difficult airway?
4. Can I use RSI?
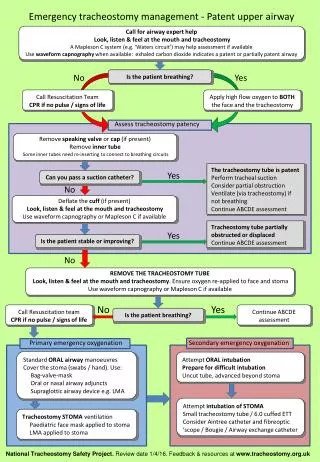
5. Outline Indications for intubation
Basic airway algorithm
Difficult airways
Difficult airway algorithm
Securing the difficult airway
Cases
6. Outline Indications for intubation
Basic airway algorithm
Difficult airways
Difficult airway algorithm
Securing the difficult airway
Cases
7. Indications for Intubation Failure of oxygenation
Failure of ventilation
Failure to protect
Impending obstruction
Expected management
8. Failure of Oxygenation
Low FiO2
Failure of ventilation
V/Q mismatch
Diffusion abnormalities
Anemia
Low C.O.
Increased tissue O2 consumption
9. Failure of Ventilation Brain; CHI
Stroke
Raised ICP
Stem; Stroke
Narcotics
Injury
Cord; SCI
Degenerative diseases
Nerve; Peripheral Neuropathy
NMJ; Myasthenia gravis
Guillon-Barre
NMJBs
Muscle; Myopathy
Thorax; Burn eschar
Rib fractures
Lungs; Restrictive disease
Contusions
Abdomen; Tense ascities
Compartment Syndrome
10. Failure to Protect Low or dropping GCS
�GCS less than 8, intubate�
Aspiration risk
11. Impending Obstruction
Expanding hematoma
Deep space infection
Epiglotitis/Bacterial tracheitis
Angioedema/Allergic reaction
Inhalation injury
Eschar
Foreign body
Tumour
Others�.
12. Outline Indications for intubation
Basic airway algorithm
Difficult airways
Difficult airway algorithm
Securing the difficult airway
Cases
13. Basic airway algorithm
14. The 8 �P�s of RSI 0 - 10min Preparation
0 - 5 min Preoxygenation
0 � 3 min Premedication
0 Pharmacological Induction
0 Pressure
0 Paralysis
0 + 45 sec Place tube
0 + 1 min Post Intubation Care
15. Outline Indications for intubation
Basic airway algorithm
Difficult airways
Difficult airway algorithm
Securing the difficult airway
Cases
16. Difficult Airways Difficult mask ventilation
Difficult laryngoscopy
Difficult tracheal intubation
Combinations of above
17. Difficult Airway EMS Incidence;
Not known
ED Incidence;
Not known
Cricothyrotomy reported as high as 1%
Definitely inflated
Reflects an aggressive approach without employing alternate intubation techniques
18. Difficult Airways Difficult mask ventilation;
Predicting the difficulty (BOOTS);
Bearded
Older (> 55 years)
Obese (BMI > 26 kg/m2)
Toothless
Snores
19. Difficult Airways Difficult laryngoscopy/intubation;
Predicting the difficulty (LEMON);
Look
Evaluate; 3,3,2
Mallampati score
Obstruction
Neck mobility
20. Difficult Airways The airway assessment;
Look (BOOTS, others)
Evaluate; 3,3,2
Mallampati score
Obstruction
Neck mobility
28. Evaluate 3:3:2
29. Mallampati score
32. Neck Mobility
34. Difficult Airways Specific situations;
Trauma
Obesity
Pregnancy
Pediatrics
35. Difficult Airways Not a catastrophe if you can�t see well
Not even if you can�t intubate
But, if you ALSO can�t ventilate��.
37. Outline Indications for intubation
Basic airway algorithm
Difficult airways
Difficult airway algorithm
Securing the difficult airway
Cases
39. Outline Indications for intubation
Basic airway algorithm
Difficult airways
Difficult airway algorithm
Securing the difficult airway
Cases
40. Securing the Difficult Airway Anticipated;
Best to get patient to ED/OR
BVM as bridge
Otherwise intubation
Don�t burn bridges
42. Securing the Difficult Airway Unanticipated;
Can you ventilate??
Yes = time
No = trouble
44. Difficult Airways Difficult ventilation;
1. Head tilt/chin lift
2. Exaggerated Jaw thrust
3. Oral/nasal airways
4. Two handed/two person technique
5. Consider mask change
6. Ease up on cricoid pressure
7. Rule out FB
53. Outline Indications for intubation
Basic airway algorithm
Difficult airways
Difficult airway algorithm
Securing the difficult airway
Cases
54. Case 1 13 yr/o M mountain biking
Neck vs. handlebars
Sitting-up on bike path
Anterior neck swelling
VSS
Mild stridor
How will you proceed?
55. Case 2 40 yr/o M
Fall from height
Spike through mandible into eye
HD stable, respiratory distress
Gaping mandible and bleeding into airway
GCS 14
How will you proceed?
56. Case 3 67 yr/o F
Sudden collapse
On ship in Southern Ocean (Antarctica)
Decreased LOC, blown pupil, posturing
GCS 6�.5�.4�.
40 220/110 16 100% 37.0
How will you proceed?
57. Case 4 30 yr/o M
Hanging two feet off ground
Found unconscious
Now agitated
Anterior neck;
rope mark
Swelling
++ tender
How will you proceed?
58. Case 5 40 yr/o F
Extensive full thickness burns;
Head, face
Neck, thorax, and arms circumferentially
VSS
GCS 15
Gross stridor
How will you proceed?
59. Case 6 30 y/o male
Shotgun blast to face
Bleeding and gross disruption of anatomy
GCS 15
VSS
How will you proceed?
60. The 4 Questions Does this patient need intubation now?
Is this a crash situation?
Is this a difficult airway?
4. Can I use RSI
62. Securing the Difficult Airway Anticipated;
Best to get patient to ED/OR
BVM as bridge
Otherwise intubation
Don�t burn bridges
63. Difficult Airways Difficult ventilation;
1. Head tilt/chin lift
2. Exaggerated Jaw thrust
3. Oral/nasal airways
4. Two handed/Two person technique
5. Consider mask change
6. Ease up on cricoid pressure
7. Rule out FB
64.
Questions?