Download
1 / 50
660 likes | 1.02k Views
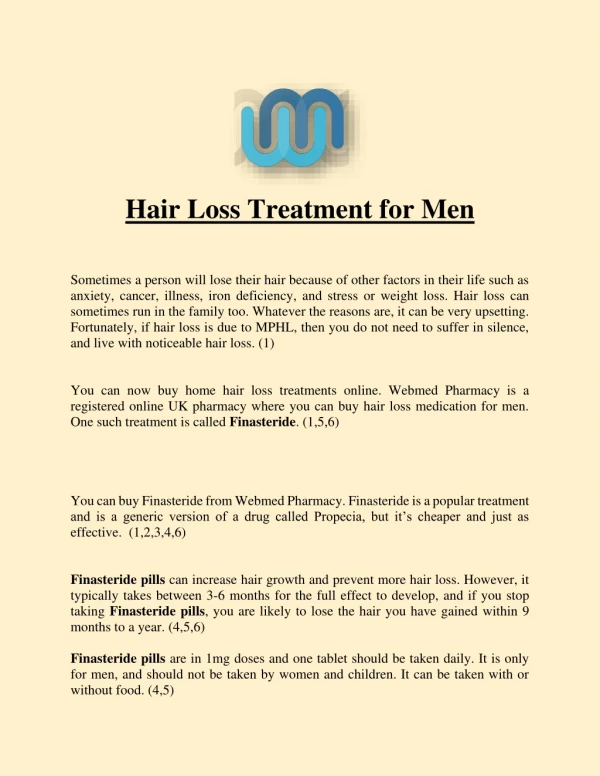
Androgenetic Alopecia (Male and Female Pattern Hair Loss). ALI ASILIAN PROF OF DERM ISFAHAN UNI OF MED SCI. HAIR AND HAIR FOLLICLE. AREAS WITHOUT HAIR:. NUMBER OF HAIRS. Scalp : about 1,00,000 hairs. Face : about 600 hairs /cm 2 . Rest of the body : about 60 hairs/cm 2.

E N D
Androgenetic Alopecia (Male and Female Pattern Hair Loss) ALI ASILIAN PROF OF DERM ISFAHAN UNI OF MED SCI
NUMBER OF HAIRS Scalp : about 1,00,000 hairs. Face : about 600 hairs /cm2. Rest of the body : about 60 hairs/cm2.
. X Alopecia None Scaring (Reversible) Scaring (Irreversible)
CLASSIFICATION OF ALOPECIA • FOCAL HAIR LOSS • Non-Scarring: A. Abnormality of cycling- i. Alopecia areata. ii. Syphilitic alopecia. B. Production decline- i. Androgenetic alopecia. ii. Triangular alopecia.
FOCAL HAIR LOSS(Contd.) C. Hair breakage- i. Trichotillomania. ii. Tineacapitis. iii. Traction alopecia. iv. Primary or acquired hair shaft abnormality.
Figure 2. Hair shedding scale. Sinclair R, Torkamani N and Jones L 2015 [version 1; referees: 4 approved] F1000Research 2015, 4:585 (doi: 10.12688/f1000research.6401.1)
Figure 4. Normal scalp. Sinclair R, Torkamani N and Jones L 2015 [version 1; referees: 4 approved] F1000Research 2015, 4:585 (doi: 10.12688/f1000research.6401.1)
Figure 10. Scalp follicles exist as compound follicular units. Sinclair R, Torkamani N and Jones L 2015 [version 1; referees: 4 approved] F1000Research 2015, 4:585 (doi: 10.12688/f1000research.6401.1)
Clinical features - FPHL The most common pattern of FPHL is diffuse central thinning of the crown with preservation of the frontal hairline. Often there is frontal accentuation of the hair loss, creating a "Christmas tree" pattern]
Figure 6. In androgenetic alopecia, a reduction in the number of hairs per follicular unit precedes the... Sinclair R, Torkamani N and Jones L 2015 [version 1; referees: 4 approved] F1000Research 2015, 4:585 (doi: 10.12688/f1000research.6401.1)
Androgenetic Alopecia • Androgenetic Alopecia affects up to 50% of males and 40% of females • Autosomal dominant with variable penetrance • 85% : +ve family history • Role of androgens in the pathogenesis:
Systemic Treatment 5 ALPHA Reductase X Fenastride Testosterone DihydorTestosterone (Active) Miniaturization of Terminal Hairs
ANDROGENETIC ALOPECIA Synonyms : Male Pattern alopecia, Male pattern baldness, Common baldness Secretarial alopecia. Definition : It is a very common, potentially reversible scalp hair loss that generally spares parietal and occipital areas (Hippocratic wreath) of the scalp.
ANDROGENETIC ALOPECIA (Contd.) Age : Twenties or early thirties. sites : Chiefly vertex and frontotemporal regions. Etiopathogenesis: • Exact mechanism is still unknown. • Hereditary (Probably autosomal dominant) & • Androgen (specifically dihydrotestesterone)
ETIOPATHOGENESIS (Contd.) Testesterone5RDihydrotesterone. • 5R has two Isozyme, 5R1 and 5R2 • 5R1 ubiquitously distributed in skin particularly in sebaceous gland. • 5R2 is found in outer root sheath and dermal papillae.
ANDROGEN Androgen - androgen receptor complex in cytoplasm transformation of receptor to expose DNA binding domain binds to androgen response element of DNA Transcription and translation certain effector protein,
ETIOPATHOGENESIS (Contd.) EFFECTS - Shortening of anagen and lengthening of telogen - Follicle become short and sclerosis of dermis and miniaturization or reduction of hair present.
CLINICAL FEATURE • Hair loss starts any time after puberty “Whisker hairs” – first sign of impending male pattern alopecia, appear at the temple. • “Professor’s angle” – anterior hair line recedes backward on each side. • Eventually entire top of the scalp become devoid of hair.
Clinical features - MPHL AGA based upon frontoparietal and frontalrecession as well as vertex thinning (see Fig. 157.2). Occasionally, a "male type" pattern with frontotemporal and vertex thinning is seen in women, and then they too can be classified with the Hamilton or NOlwood system.
Figure 1. Sinclair scale for female pattern hair loss. Sinclair R, Torkamani N and Jones L 2015 [version 1; referees: 4 approved] F1000Research 2015, 4:585 (doi: 10.12688/f1000research.6401.1)
Androgenetic alopecia in women Etiology : • Genetic Predisposition, • Androgen excess, Ovarian cause- - Polycystic ovarian syndrome, - Other ovarian tumor, . Unilateral benign microadenoma. . Leydig cell tumor . Hilar cell tumor.
ETIOLOGY (CONTD.) • Adrenal cause - Congenital adrenal hyperplasia (androgenital syndrome) due to deficiency of – 21 hydroxylase (most common) 11-β hygroxylase. 3-β hydroxysteroid dehydrogenase. - Tumor Adrenal adenoma Carcinoma.
CLINICAL FEATURE Pattern of hair loss : “Christmas tree pattern”- diffuse and progressive reduction of density and diameter of hairs in the mid scalp. • Maintenance of frontal hair lines with onlyslight recession.
CLINICAL FEATURE (CONTD.) • Other evidence of androgen excess: • Acne. • Hirsutism. • Menstrual irregularities. • Majority of women with pattern hair loss have • No increased serum androgen, • No other sign symptom of androgen hypersensitivity.
Pathology Androgenetic alopecia with the characteristic miniaturization of hair follicles Androgenetic alopecia at the level of the isthmus with miniaturized vellus-like hair follicles and no significant inflammation
B: Normal scalp (horizontal section). C: Androgenetic alopecia with variation in hair follicle size (horizontal section; compare to B)
Figure 3. Horizontal section of skin biopsy from a hairy scalp showing features of early androgenetic... Sinclair R, Torkamani N and Jones L 2015 [version 1; referees: 4 approved] F1000Research 2015, 4:585 (doi: 10.12688/f1000research.6401.1)
Figure 5. Horizontal section of skin biopsy from a hairy forearm showing follicles to exist singly or... Sinclair R, Torkamani N and Jones L 2015 [version 1; referees: 4 approved] F1000Research 2015, 4:585 (doi: 10.12688/f1000research.6401.1)
Figure 8. In androgenetic alopecia, the proximal arrector pili muscle (red) is progressively replaced... Sinclair R, Torkamani N and Jones L 2015 [version 1; referees: 4 approved] F1000Research 2015, 4:585 (doi: 10.12688/f1000research.6401.1)
TREATMENT 1. Topical Minoxidil (2% & 5%) -non specific hair growth promoter affecting anagen induction. - M/A is not clear, its ca channel opener activity is important. 2. Systemic Finesteride (1mg daily).
TREATMENT (CONTD.) 3. In women – spironolactone ( >100 mg daily). - Flutamide (250-500 mg bid or tid). - Cyproteroneactate. 4. Surgical treatment- Micrograft & minigraft from non-androgen dependent site (occiput).
alternatives for the treatment • hair transplantation • scalp reduction
هزاران معنی باریک باشد بیت ابرو را به غیر از مو شکافان کس نداند معنی او را