
Equivalence of Doctor Interactions Between Activator Methods and Sham Chiropractic Protocols During an Expertise-Based Randomized Controlled Trial.

E N D
Presentation Transcript
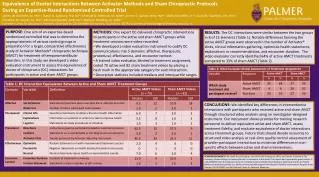
Equivalence of Doctor Interactions Between Activator Methods and Sham Chiropractic Protocols During an Expertise-Based Randomized Controlled Trial • James W. DeVocht, DC, PhD(1); Stacie A. Salsbury, PhD, RN(1); Michael B. Seidman, DC, MSW(1); Lynne A. Carber, MPM, PMP(1); Wally Schaeffer, DC(2); Clark M. Stanford, DDS, PhD(3); Christine M. Goertz, DC, PhD(1); Michael Spector, DMD, MS(3); Maria A. Hondras, DC, MPH(1) • (1) Palmer Center for Chiropractic Research, Davenport IA; (2) Schaeffer Chiropractic, Coralville IA; (3) The University of Iowa College of Dentistry, Iowa City, IA PURPOSE: One aim of an expertise-based randomized controlled trial was to determine the appropriateness of various control groups in preparation for a larger, comparative effectiveness study of Activator Methods® chiropractic technique (AMCT) for treatment of temporomandibulardisorders. In this study, we developed a video evaluation instrument to assess the equivalence of doctor of chiropractic (DC) interactions for participants in active and sham AMCT groups. • METHODS: One expert DC delivered chiropractic interventions to participants in the active and sham AMCT groups while treatment sessions were video-recorded. • We developed a video evaluation instrument to codify DC communications into 5 domains: affective, therapeutic, procedural, effectiveness, and encounter context. • A trained video evaluator, blinded to treatment assignment, coded 70 active and 82 sham treatment videos by placing a hash mark in the appropriate category for each interaction. • Descriptive statistics included medians and interquartile ranges. RESULTS: The DC interactions were similar between the two groups in 8 of 13 elements (Table 1). Notable differences favoring the active AMCT group were observed in the number of Activator® clicks, clinical information gathering, optimistic health statements, explanations or recommendations, and encounter duration. The video evaluator correctly identified 64% of active AMCT treatments compared to 33% of sham AMCT (Table 2). CONCLUSIONS: We identified key differences in interventionist interactions with participants who received active and sham AMCT through structured video analysis using an investigator-designed instrument. Our instrument shows promise for training research personnel to deliver equivalent active and sham AMCT, assess treatment fidelity, and evaluate equivalence of doctor interactions across treatment groups. Future trials should devote resources to structured video analysis or real-time quality control assessment of provider-participant interactions to minimize differences in non-specific effects between active and sham interventions. ACKNOWLEDGEMENTS: We thank the participants, the staff at the chiropractic office, and Lauren Thomann at The University of Iowa College of Dentistry for their involvement in this study. This project was supported by grant number 1-U19-AT004663 from the National Center for Complementary and Alternative Medicine, National Institutes for Health (NIH)) and conducted partially in a facility constructed with support from Research Facilities Improvement Program Grant Number C06 RR15433 from NIH National Center for Research Resources.