Drugs for Asthma
300 likes | 897 Views
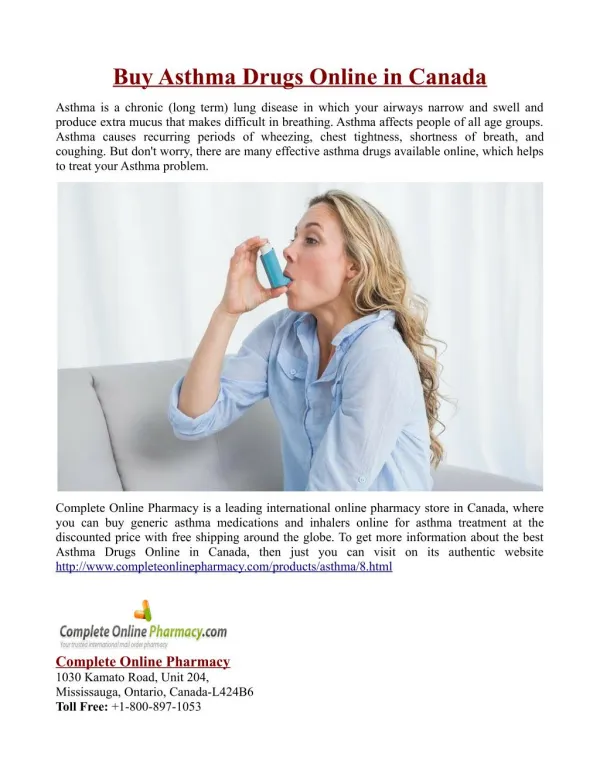
Drugs for Asthma . Francesca Burns. Aims and objectives. Understand regulation of airway muscle Pathophysiology of asthma Step-wise management Pharmacology of each drug class Emergency Mx acute asthma attack. Hallmarks of asthma. Intermittent and reversible airway obstruction

Drugs for Asthma
E N D
Presentation Transcript
Drugs for Asthma Francesca Burns
Aims and objectives • Understand regulation of airway muscle • Pathophysiology of asthma • Step-wise management • Pharmacology of each drug class • Emergency Mx acute asthma attack
Hallmarks of asthma • Intermittent and reversible airway obstruction • Chronic bronchial inflammation with eosinophils • Bronchial smooth muscle cell hypertrophy and hyperractivity • Increased mucus secretion
Regulation of airway muscle, blood vessels and glands Respond to exogenous chemicals, inflammatory mediators and physical stimuli Irritant receptors & C-fibres Afferent pathways Bronchoconstriction and mucus secretion Muscarinic (M3) Parasympathetic Efferent pathways Autonomic innervation β2- adrenoceptors Sympathetic Relax airway smooth muscle Cause neuroinflammation NANC + Cause relaxation -
Pathophysiology: Reversed by β2 adrenoceptor agonists, leukotriene receptor antagonist and theophylline Bronchoconstriction Early phase Increased mucus Vasodilation 2 phases Activation and recruitment of leukocytes Late phase Inflammation Inhibited by glucocorticoids Airway remodelling
Drugs • 2 categories: • Bronchodilators • Anti inflammatory agents
β2 agonist • Mechanism of action: • increase intracellular cAMP leading to smooth muscle relaxation and bronchodilation • Inhibition of mediator release from mast cells • Enhanced mucociliary clearance • Pharmacokinetics: • Administration: inhaler, nebuliser or IV • Short acting: max effect within 30 mins, last 3-5 hours • Long acting: last 8-12 hours • Metabolised by liver
Indications: • Acute asthma (short acting) • Chronic asthma/COPD (long acting) • Premature labour • Cautions: hyperthyroidism, cardiovascular disease, arrhythmias, susceptibility to QT-interval prolongation, and hypertension.
Fine tremor • Hypokalaemia (if high dose given) • Tachycardia – secondary to peripheral vasodilation and cardiac stimulation • Headache • Side effects:
Steroids • Mechanism of action: anti-inflammatory • Decrease formation of cytokines (esp Th2) • Inhibit induction of COX-2 • Pharmacokinetics: • Administration: inhaled or oral • t = variable (12-36 pred, 8-12 hydrocortisone) • Metabolised predominantly in liver
Side effects: • Oropharyngeal candidiasis • Bruising and impaired healing • Osteoporosis • Peptic ulcerations • Increased susceptibility to infections • …….. • Cautions: pregnancy and in growing children
Leukotriene receptor antagonist(e.g.Montelukast, zafirlukast) • Mechanism of action: block action of cysteinylleukotrienes in smooth muscle , therefore inhibiting inflammation • Pharmacokinetics: • Administration: oral (Mx1D, Zx2D) • t=3-7h (montelukast) • Metabolised by liver and excreted by biliary route • Indications: • Asthma (step 3) • Seasonal allergic rhinitis
Cautions: • In patients taking liver inducing drugs • Phenobarbitol use reduces plasma levels • Avoid in P&B unless essential • Side effects: • Abdo pain • GI disturbance • Headache • Churg Strauss
SR TheophyllineA methylxanthine • Mechanism of action: inhibits phosphodiesteraseisoenzymes resulting in increased cAMP levels and smooth muscle relaxation bronchodilatory effect. • Pharmacokinetics: • Administration: oral • t= 8 hours • Metabolised by liver (CP450) and excreted by kidneys • Indications: • Acute severe asthma • Chronic asthma • Moderate to severe COPD
Cautions: • Porphyria • Concomitant use of ephedrine in children • Cardiac or liver failure and poorly controlled epilepsy • t reduced by smoking, heavy drinking and p450 inducers • Monitor K+ levels • Side effects: • Hypokalaemia • Tachycardia, palpitations, and arrthymias • Headache and insomnia • GI disturbances • Convulsions
Inhaled antimuscarinicsIpatropium bromide • Mechanism action: • competitive agonists of Ach in bronchial smooth muscle. • Bind and block M3 receptors • Therefore prevent smooth muscle contraction and consequent airway constriction • Pharmacokinetics: • Given by aerosol inhalation • Max effect at 30 mins, t 1.6 hours • Excreted in urine
Cautions: prostatic hyperplasia, bladder outflow obstruction, and those susceptible to angle-closure glaucoma • Indications: asthma • Side effects: • Dry mouth • Nausea • Headache
Management of Acute Asthma attackOh – S H I T ! • O - Oxygen • S – Salbutamol (nebuliser, followed by course of oral prednisolone) • H – Hydrocortisone (IV) • I - Ipatropium • T – theophylline (or MgSO4)
Last thing…Aspirin induced asthma • 5% individuals with asthma experience exacerbations when they take aspirin or other NSAIDS. • Samters triad: Asthma, aspirin sensitivity, nasal polyps • Common in middle aged men • This occurs because aspirin is a mixed COX-1 and COX-2 inhibitor, reducing PG2 and increasing leukotriene synthesis…causing bronchospasm. • Prior learning: Ali teach
Questions • 1. A 33-year-old man is seen in the asthma clinic. He was referred with poorly control asthma and has recently had salmeterol added in addition to beclometasonedipropionate inhaler 200mcg bd and salbutamol prn. There has unfortunately been no response to adding the salmeterol. What is the most appropriate action? • Stop salmetarol and trial of leukotriene receptor antagonist • Continue salmeterol + increase beclometasonedipropionate inhaler to 400mcg bd • Continue salmeterol + trial of leukotriene receptor antagonist • Stop salmeterol + trial of oral theophylline • Stop salmeterol + increase beclometasonedipropionate inhaler to 400mcg bd
A 45-year-old woman who is a known asthmatic comes for review. In the past two years she has had around six exacerbations of asthma requiring oral steroids. Her current medication includes salbutamol 2 puffs prn, salmeterol 50mcg bd and beclomethasone 200 mcg 1 puff bd. You note from the records that her BMI is 31 kg/m^2, she is a non-smoker and has a good inhaler technique. What is the most appropriate next step in management? • Increase beclomethasone to 200 mcg 2 puffs bd • Referral to a dietician • Add oral theophylline • Add oral montelukast • Add inhaled tiopropium
Which of the following are common adverse effects of B2 agonists? • A) Tremor • B)Bradycardia • C) Ankle oedema • D)Tachycardia • E)Oral Candidiasis