Download
1 / 14
290 likes | 902 Views
MYASTHENIA GRAVIS. “FROM WEAKNESS SHALL COME STRENGTH”. BY PATTI HAMILTON. Who gets MG? All ethnic groups Most commonly young women (under 40) and older men ( over 60), but it can occur at any age. It is not inherited nor is it contagious.

E N D
MYASTHENIA GRAVIS “FROM WEAKNESS SHALL COME STRENGTH”. BY PATTI HAMILTON
Who gets MG? All ethnic groups Most commonly young women (under 40) and older men ( over 60), but it can occur at any age. It is not inherited nor is it contagious. Famous people include – David Niven, Aristotle Onassis, Sir Lawrence Olivier, Phil silvers, and Sleepy . Sleepy was supposedly based on a friend of Walt Disney who had MG. Myasthenia Gravis – definition – from greek and latin means “grave muscle weakness”.
What is Myasthenia Gravis? • Chronic autoimmune neuromuscular disease. • Characterized by varying degrees of weakness of the voluntary muscles of the body. • Hallmark sign is muscle weakness that increases with activity and improves after periods of rest.
What causes Myasthenia Gravis? What causes MG? • A defect in the transmission of nerve impulses to muscles at neuromuscular junction. • Antibodies block, alter, or destroy the receptors for acetylcholine at the NMJ which prevents the muscle from contracting. • Studies show that patients with Mg have only about one third as many acetylcholine receptors at the NMJ as is normal.
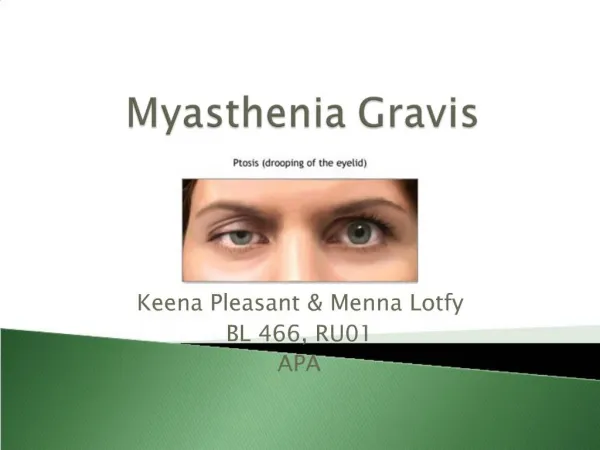
Signs and symptoms • In most cases, the 1st noticeable symptom is weakness of eye muscles. In other cases, difficulty swallowing and slurred speech may be the first sign. • Other Symptoms include and vary in type and severity, they are ptosis, diplopia, unstable and waddling gait, weakness in arms, hand, fingers, legs, neck, a change in facial expression, and shortness of breath. • The vocal cords can become weak and the voice is nasal sounding. • As the disease progresses, the patient will have trouble with walking, sustained sitting, and raising their arms over their heads. Breathing problems can become so severe they require a ventilator. Bowel and bladder sphincter weakness occurs.
Diagnostics • The simplest diagnostic test is to have the patient look up for 2 to 3 minutes. The patient with MG will barely be able to keep their eyes open. • Electromyogram • Serum testing for antibodies • Edrophonium test.
How is Myasthenia Gravis treated? • Medications include – Anticholinesterase agents which include neostigmine and pyridostigmine. Immunosuppressive drugs such as cyclophosphamide, cyclosporine, and azathioprine. Care must be taken with medications because many classes of drugs are contraindicated with patients with MG. These include anesthetics, antidysrhythmics, antibiotics, quinine, antipsychotics, barbiturates, sedatives, hypnotics, opioids, tranquilizers, and thyroid preparations.
Treatment Continued - • Plasmapheresis • Thymectomy – In adults with MG the thymus gland is abnormal. Some individuals develop thymomas which require surgical removal. ( Thymectomy reduces symptoms in more than 70% of patients without thymoma and cures some individuals). • High dose intravenous immune globulin.
Myasthenic crisis • A myasthenic crises occurs when the muscles that control breathing weaken to the point that ventilation is inadequate. This is a medical emergency and requires a respirator for assisted ventilation. • A crisis may be triggered by infection, fever, or an adverse reaction to medication.
Nursing interventions - • Airway protective techniques – Chin tuck, double swallowing. • Suctioning if necessary, for upper respiratory infections. • Medications 1 hr. before meals. • Feeding tube if swallowing is a problem. • Assess need for respiratory assistance with Serial determination of vital capacity, minute volumes, and tidal volumes.
Patient teaching • Take meds. As prescribed times and to take them early enough before eating or activities to obtain maximum relief. • Explain how to adjust medication dose to maintain muscle strength. • Medications to avoid. • Seek medical attention at first sign of URI. • Eat only when sitting up to prevent aspiration.
Teaching Continued- • Avoid crowds in flu and cold season. • Explain how to adjust daily activities to allow for leisure activities and rest periods. • To use minimal energy in ADL’s so that energy may be used for activities that patient enjoys. • Advise patient to wear medic-alert bracelet.
What is the prognosis? • With Treatment, the outlook for most patients is bright. They will have significant improvement of their muscle weakness and they can expect to lead normal or nearly normal lives. • Some patients may go into remission temporarily, so that medications can be discontinued. • In a few cases, a severe crisis (respiratory failure) may cause death.