Download

1 / 45
520 likes | 1.16k Views
HIV infection in Pregnancy. รองศาสตราจารย์ นายแพทย์ อติวุทธ กมุทมาศ สาขาสูติศาสตร์และนรีเวชวิทยา คณะแพทยศาสตร์ มหาวิทยาลัยธรรมศาสตร์. Natural history. The principal target=T lymphocytes Specific at CD4 surface antigen (receptor for the virus) Monocyte-macrophages may be infected

E N D
HIV infection in Pregnancy รองศาสตราจารย์ นายแพทย์ อติวุทธ กมุทมาศ สาขาสูติศาสตร์และนรีเวชวิทยา คณะแพทยศาสตร์ มหาวิทยาลัยธรรมศาสตร์
Naturalhistory • The principal target=T lymphocytes • Specific at CD4 surface antigen (receptor for the virus) • Monocyte-macrophages may be infected • Incubation period ; days to weeks • Acute retroviral syndrome ; fever, night sweats, fatigue, rash, headache, lymphadenophathy, pharyngitis, myalgias, arthralgias, nausea, vomiting, diarrhea ; lasts < 10 days
After symptoms abate ; chronic viremia • Median time = 10 years --- AIDS • AIDS; generalized lymphadenopathy, oral hairy leukoplakia, aphthous ulcer, thrombocytopenia, opportunistic infections (candida, HSV, TB, CMV, HPV, PCP, toxo), Kaposi sarcoma, non-Hodgkin lymphoma • Death
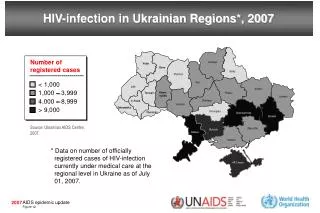
Number of People with HIV/AIDS by Region Western Europe 500,000 Eastern Europe & Central Asia 270,000 North America 890,000 East Asia & Pacific 560,000 North Africa & Middle East 210,000 Caribbean 330,000 South and South East Asia 6.7 million Sub-Saharan Africa 22.5 million Latin America 1.4 million Australia and New Zealand 12,000 Source: UNAIDS/WHO 1998.
Virology • DNA retrovirus • HIV-1 , HIV-2 • Transmission - sexually transmitted - blood-contaminated (e.g., blood transfusions, shared needles, contaminated instruments) - maternal to child -vertical 15-40% -breast feeding 30-40%
Maternal to child transmission (MTCT) 36 wk-labor <14 wk 14-36 wk Intrapartum 75 % uninfected 25 % infected 8 1 4 12 4% 16% 50% 30% Kourtis and colleagues, 2001
Risk factors for vertical transmission 1. Preterm birth (3.7 relative risk for intrapartum transmission ; Kuhn and assoc 1999) 2. Prolonged membrane rupture (increase rate from 15 to 25% in ROM > 4 hr ; Landesman and co-workers 1996) 3. Placental inflammation, chorioamnionitis, concurrent syphylis (Mwanyumba 2002)
4. Maternal plasma HIV RNA level Most important factor, HIV RNA viral load > 100000 copies/ml : risk > 30 % HIV RNA viral load < 400 copies/ml : risk 1 %
5. Stage of disease 6. CD4+ T-cell count 7. Mode of delivery cesarean section vs vaginal delivery 8. Breast feeding(risk 30-40%)
HIV infection on pregnancy Pregnancy on HIV infection • Pregnancy : slightly immunosuppressive : minimal effect on CD4 count : minimal effect on HIV RNA level : does not have significant effect on the clinical or immunological course of HIV infection (Minkoff 2003) • Maternal morbidity and mortality : not increased • Slightly increase rate of preterm birth • Slightly increase rate of IUGR • Slightly increase rate of PROM • Fetal and neonatal infection • varies from 25-40 percent
Adverse Pregnancy Outcomes and Relationship to HIV Infection Anderson 2001.
Adverse Pregnancy Outcomes and Relationship to HIV Infection (continued) Anderson 2001.
Management during pregnancy • Therapeutic goals ; maximal suppression of viral load and restoration of immunological function ; prevention of maternal to child transmission • ARV therapy should be offered to all HIV infected pregnant women regardless of CD4 cell count or HIV RNA level • To treat the mother as well as to reduce the risk of perinatal transmission • Holistic care : antepartum / intrapartum / postpartum : mother / fetus-baby : psycho / bio / social
Antepartum care • Posttest counseling / psychological support • History taking • Physical examination • Per vaginal examination • Oral health examination • Ophthalmic examination • Lab tests • Tuberculin test • Chest X-ray • Prenatal care in high risk clinic • Nutrition support / vitamin supplementation • Ultrasound • Prevention of opportunistic infection • Immunization • Anteretroviral administration
Intrapartum care • ARV during labor period ; minimum viral load • Mode of delivery • Labor augmentation is used when needed to shorten the interval to delivery / but avoid ARM • Minimize operative obstetrics : scalp electrode, fetal scalp blood sampling, forceps extraction, vacuum extraction • Universal precaution; percutaneous exposure of needle=0.3%, mucous membrane exposure=0.09%, atraumatic needle, absorbable suture, non-touch technique, 0.5% sodium hypochloride, room for isolation
Cesarean section ; decrease vertical transmission one-half compared with vaginal delivery(metaanalysis of 15 prospective cohort studies by the international perinatal HIV group 1999) • Combined cesarean section with ARV reduced the risk 87 % • ACOG 2000 ; recommended C/S when HIV RNA viral loads > 1000 copies/ml • Scheduled C/S is recommended at 38 wk • If viral load < 1000 copies/ml ; data insufficient to estimate benefit of C/S (ACOG 2000)
Postpartum care 1. ARV Mother: • AIDS, HIV infection with CD4<200 ; continue ARV treatment • CD4 200-350 ; controversial for ARV • CD4 > 350 ; stop ARV , monitoring CD4 Baby: ARV 1 / 6 weeks If delivery occurs before treatment is given, the newborn can receive prophylaxis for 6 weeks with zidovudine, or in some cases combination antiretroviral treatment 2. Contraceptives ; condom + OCP • points of interest ; TR, injectable, norplant, IUD
3. Breast feeding • Not recommended • Africa ; breast feeding with continuation of ARV prophylaxis 4. Postpartum clinic and pap smear ; 6 mo / 1 year
1. Classes of ARV drugs Guidelines for ARV in pregnancy By FDA pregnancy category classification e-text McGrawHill Cunningham FG, Leveno KJ, Bloom SL, Hauth JC, Gilstrap III L, Wenstrom KD. Williams Obstetrics. 22nd ed. New York: McGRAW-HILL; 2005.
NRTI/ NNRTI PI FI
2. Regimens • NNRTI-based • PI-based • Triple NRTI-based • FI-based • http://AIDSinfo.nih.gov
3. Monitoring • CD4 count at initiation then CD4 count every 3 months • HIV RNA levels at 4 weeks after initiation of treatment then HIV RNA levels monthly until undetectable, then every 3 months • HIV RNA level at GA 36 weeks
Short course ZDV / SD NVP Short course ZDV NVP-NVP P-P NVP-NVP P-NVP NVP-P HIVNET012 ; Guay, Lancet 1999;354:795-802. PHPT-2; Lallemant, NEJM 2004; 351: 217-8. MASHI; Shpiro , AIDS 2006; 20: 1281-8. Short course AZT ; TR 8% (ACTG076)
NVP concentration after SD-NVP • Median T1/2 =61.3 hours • Drug can be detected up to 19 days • Lower limit assay quantification 50 ng/ml ; 3-4 weeks postpartum • Cressey TR. JAIDS 2005; 38: 283-8. • SD NVP covering the tail; ZDV/3TC 7 days : reduce resistance from 60 % to 10-12 % • TOPH Trial, SA
Two drugs regimen • Short course AZT (28 week)+SD NVP : TR 6.3% (PHPT-2) • AZT+ddI (36 wk to 1 wk PP) : TR 6.9% (SIMBA trial) • AZT+3TC 32 wk add SD NVP : TR 4.7% (Ditrame Plus) • AZT 36 wk + SD NVP : TR 6.5%
HAART • Depend on immune status of mother -low CD4 <200 ; start for maternal health -high CD4 ; consider -pro ; low TR (PACTG316, TR 1.5%) -con ; high risk of NVP toxicity, increase risk of GDM with PI, risk of preterm delivery (controversial) • Which HAART? -NNRTI based HAART -PI based HAART
Toxicities concerned • NVP -rash ; women>men (3.7 x) -more common with high CD4 > 250 (10X increase in women) • Hepatotoxicity -symptomatic hepatotoxicity ; CD4 <250 :0.5-1.7%, CD4 > 250: 10.0-11.3% -fetal hepatic events ; CD4 250-400 : 0.42%, CD4 >400 : 1.1%) -TRC cohort ; low : high CD4 2.9% versus 7.7%
5. Factors for selection Mother Child Medical services
ทีมงาน • อายุรแพทย์ (อ.อนุชา) • สูติแพทย์ (อ.อติวุทธ) • กุมารแพทย์ (อ.อัจฉรา) • ทีมพยาบาลหน่วยเอดส์ธรรมศาสตร์ (คุณกรองทิพย์) • ทีมอาสาสมัครผู้ติดเชื้อ (คุณวันใหม่) • เภสัชกร • นักสังคมสงเคราะห์ • อื่น ๆ
< 2540 ; no ARV important role of a termination of pregnancy • 2541-2546 ; AZT + SD NVP • > 2547 ; HAART
ข้อมูลจาก หน่วยเอดส์ธรรมศาสตร์ โรงพยาบาลธรรมศาสตร์เฉลิมพระเกียรติ
AZT regimen • Prevalence of HIV infection pregnancy in TUH = 1-2 percent • AZT alone= infection rate 3.9 percent • AZT regimen from other studies ; infection rate 5-8 percent, ACTG 076 protocol = 8% • Cesarean section = beneficial • MPH ; still using AZT regimen
Regimens; Pediatrics AIDS clinical trials group, USA • Antepartum: 100 mg 5times/day, initiating at 14-34 wk,continuethroughout pregnancy(or 200 mg 3times/day, 300 mg twice a day) • Intrapartum: IV Zidovudine in a 1-hr initial dose of 2 mg/kg, followed by a continuous infusion of 1 mg/kg/hr until delivery • Neonates: begin at 8-12 hr after birth, and give syrup at 2 mg/kg every 6 hr for 6 weeks
Regimen MPH • Antepartum; 300 mg twice a day, initiating at 14-34 (28) wk,continuethroughout pregnancy (regardless of CD4 count) • Intrapartum; AZT 300 mg every 3 hr and single dose NVP 200 mg orally • Postpartum; AZT 300 mg+3TC 150 mg twice a day for 2 weeks • Neonates; NVP 2 mg/kg single dose and AZT 2 mg/kg every 6 hr for 6 weeks • Disadvantages (compare to HARRT) : • Higher transmission rate • High incidence of NVP resistance
HAART (AZT+3TC+NVP) ข้อมูลจาก หน่วยเอดส์ธรรมศาสตร์ โรงพยาบาลธรรมศาสตร์เฉลิมพระเกียรติ
Triple agents (HARRT) Thammasat Hospital ; transmission rate1.2 % • Other studies ; transmission rate 1-1.5%
Regimen : TUH 1. CD4 ≤ 200 / GA 14 weeks • Antepartum; AZT(300)/3TC(150) q 12 hr + NVP(200) OD for 2 wk then AZT(300)/3TC(150) +NVP(200) q 12 hr • Intrapartum; AZT 300 mg q 3 hr and AZT(300)/3TC(150) +NVP(200) q 12 hr • Postpartum; AZT(300)/3TC(150) +NVP(200) q 12 hr • Neonates; AZT 2 mg/kg q 6 hrx6 wk
2. CD4> 200 / GA 28 weeks • Antepartum; AZT(300)/3TC(150) q 12 hr + NVP(200) OD for 2 wk then AZT(300)/3TC(150) +NVP(200) q 12 hr • Intrapartum; AZT 300 mg q 3 hr and AZT(300)/3TC(150) +NVP(200) q 12 hr • Postpartum; AZT(300)/3TC(150) q 12 hr x 14 days, stop NVP • Neonates; AZT 2 mg/kg q 6 hrx6 wk
Alternative regimens; • AZT/3TC/Nelfinavir(NLF) (250 mg 5 tabs q 12 hr, no need for test dose, no covering tail) • AZT/3TC/Efavirenz (GA>24wk) • GPOvir(3TC/d4T/NVP)(follow the protocolAZT/3TC/NVP and test doses NVP for 2 wk) In case C/S • Start AZT with 30 cc of water since NPO then NPO except medicine with water until delivery and postop care period 12-24 hr For no ANC patients • Intrapartum; AntiHIV stat, NVP 200 mg single dose (immediately) and AZT 300 mg q 3 hr regardless of CD4 count • Postpartum;AZT300/3TC150 q 12 hrx14wk • Neonates; NVP 2 mg/kg single dose + AZT 2 mg/kg q 6 hr x 6 wk (start immediately)