Benign oesophageal disease
760 likes | 1.02k Views
Benign oesophageal disease. 10-30% of patients with suspected angina don't have coronary disease. From these 50% will have oesophageal disorders. Anatomy. - Muscular tube - Conduit from the pharynx to the stomach - C6 (Cricoid cartilage) to below the diaphragm

Benign oesophageal disease
E N D
Presentation Transcript
10-30% of patients with suspected angina don't have coronary disease. From these 50% will have oesophageal disorders.
Anatomy - Muscular tube - Conduit from the pharynx to the stomach - C6 (Cricoid cartilage) to below the diaphragm - From the incisor 40-45 cm (actual 20-25cm) - Passes behind aortic arch and left main bronchus. - Enters abdomen through oesophageal hiatus → 2-4 cm below the diaphragm
Anatomy - Held in position by: . Reflection of the peritoneum onto the stomach . Phreno-oesophageal ligament to the oesophagus .
Anatomy Three area of narrowing - Cricopharangeus - Behind the aortic arch - LOS (thickening of the circular muscles ~ 4cm) The muscles upper 1/3 of oesophagus is striated, remainder is smooth muscle peristalsis wave 4-6cm/s (reflex regulated in the medulla)
Arterial supply: Venous drainage: Upper → inferior thyroid artery Middle → Bronchial arteries and oesophageal branches directly from aorta Lower → L inferior phrenic and gastric Upper → oesophageal venous plexus to azygos vein Lower → oesophageal branches of the coronary vein, a tributary of the portal vein
Histology: - Stratified columnar epithelium with scattered mucus glands - No serosa hence does not heal as well as the rest of GIT - Lower Oesophageal Sphincter (LOS) Contraction: α-adrenergic & cholinergic Gastrin Relax: β-adrenergic,VIP and NO CCK & glucagon
Symptoms: - Dysphagia: difficulty swallowing - Odynophagia: pain on or painful swallowing - Globus: lump in the throat - Heart burn: Stomach/Substernal burning sensation radiating up to the neck and relieved acutely (but transiently) by antacids
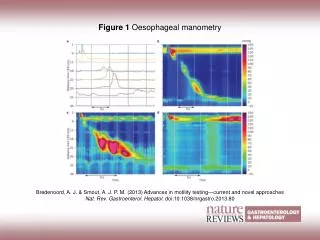
Oesophageal Motility Disorders(1) (i) Achalasia (ii) Others Diffuse oesophageal Spasm Nutcracker Oesophagus Hypertensive LOS Scleroderma & other collagen- vascular disorders (eg CREST)
Diffuse oesophageal Spasm - 3-5% of motility disorders - Normal peristalsis + Spontaneous contraction + increase in LOS pressure - Aetiology is unknown, ? defect in neural inhibition normally mediated by NO - Hypersensitive oesophagus - Dx on Manometry - Endoscopy is unremarkable & Ba Swallow is N or disorganised (Corckscrew)
Nutcracker Oesophagus Hypertensive LOS - High amplitude peristaltic waves (>180mmHg) prolonged (>6s) - Endoscopy unremarkable but Endo US shows thickening of muscularis propria - Higher incidence of psychiatric disorders - Elevated LOS pressure (>45mmHg) with normal peristalsis - LOS relaxation is normal
Treatment - Medical Rx effective in 80% - Agents acting on Smooth Muscle (eg Nitrates, Ca channel blockers), - Psychoactive agents (eg Benzodiazepines, Tricyclics) (?more effective) - Botox injection - Surgical Rx, reserved for Px with dysphagia and poor oesophageal emptying Myotomy (Lap / Thoracoscopic)
Ineffective motility - Scleroderma (80% of Px), other Collagen Vascular disorders (SLE, RA, MCTD), Amyloidosis, Alcoholism, MS, myxoedema etc - Affect the myenteric plexus + fibrosis and vascular obliteration (Predominantly distal SM) - ↓ or absent peristalsis and LOS pressure
Achalasia - Uncommon (0.5-1 in 100,000), M=F, 20-50s - Ineffective relaxation of the LOS combined with loss of oesophageal peristalsis → impaired oesophageal emptying and gradual dilatation - ↓ or loss of inhibitory myenteric ganglion cells & progressive neural fibrosis - Also decreased production of NO & VIP - Slight increase risk of SCC
Achalasia - Presentation - Dysphagia - delayed and progressive presentation (mean 2 years) - Stress or cold fluid exacerbates symptoms - Spontaneous or forced regurgitation of undigested food - 10% will have pulmonary complication - Can have heartburn (not GORD) - Chest pain (≠ heartburn) - 30-50% resolves with Myotomy
Achalasia - Diagnosis - Air fluid levels on plain Xray - Ba swallow: dilated oesophagus with Bird's beak tapering - Manometry is gold standard . Resting LOS pressure is usually normal (may be elevated) . Complete absence of peristalsis - Endoscopy: dilated oesophagus with tightly closed LOS gentle pressure will admit the scope with a "pop“.
Achalasia - Treatment - Palliation of dysphagia → relieve functional obstruction of distal oesophagus (neuromuscular defect is not corrected) Medical (Nitrates and Ca channel blockers) . Poorly absorbed, inconsistent and short lived effect . SE.
Achalasia - Treatment - Botox injection: bind to cholinergic nerves and irreversibly inhibit Acetyl Choline release - 60-85% of patient get relief but 50% get recurrent symptoms within 6 months. - Efficacy decreased with repeated injection - Expensive - Cause intense inflammatory reaction which will make subsequent surgery more difficult and increase risk of perforation.
Achalasia - Treatment - Graded pneumatic dilatation (under fluoroscopy) Tears the muscle (myotomy) 30mm for 1-3min (day procedure) Can have repeated dilatation 60-90% success rate Efficacy is decreased after second dilatation perforation rate ~ 2%
Achalasia – Surgical treatment - Originally performed by Ernest Heller in 1914 for Achalasia Two myotomies: anterior and posterior - Modified Heller: anterior only - Excellent results in 90-95% - Traditionally trans-thoracic or trans-abdominal - Now minimally invasive Laparoscopic / Thoracoscopic
Achalasia – Surgical treatment - Controversies Length of myotomy Proximal 5-7 cm above GOJ ? evidence(1) longer gastric myotomies (>3cm) better relief from dysphagia Need for antireflux procedure as well
Benign oesophageal tumours - From any layer - Mucosal: . Papillomas (sessile or pedunculated) - Intramural: . Leiomyoma, Fibroma Lipoma . Congenital cysts or reduplication (lower)
Benign oesophageal tumours - Asymptomatic or may be large enough to encroach the lumen - Peristalsis is normal with Leiomyoma, but spasm with cysts and reduplication - Intraluminal lesions Dx on Endoscopy (should Bx) - Intramural lesions Dx Radiologically (smoothly rounded) should not be Bx
Gastro-oesophageal reflux disease - Reflux of gastric content is normal - GORD is when affects patient’s well being . Symptoms . Physical complications - Common - (difficult to assess - Px self treat) - 75% of oesophageal disease in clinical practice In the US(2)40% monthly 14% weekly (15-20% Australia) 7% daily
Gastro-oesophageal reflux disease Pathogenesis: - Excessive exposure and reduced clearance of gastric content - Competent LOS Resting pressure >6mmHg Abdominal location of LOS (>1cm) (diaphragmatic crura and intra abdominal pressure) Total length >2 cm - Recurrent / prolonged relaxation
Gastro-oesophageal reflux disease - Normal gastric emptying - Adequate oesophageal clearance - Contributing Factors: Familial, Obesity, Diet (Fat, Chocolate, Caffeine), Smoking, Drugs - Hiatus hernia 85% of Px with reflux have a sliding hernia But most people with a sliding hernia don’t have disabling symptoms
Gastro-oesophageal reflux disease Symptoms Mild / Severe - Heartburn (also in PUD and 40% IBS Px) - Regurgitation of previously ingested food - Waterwash (saliva production) - Dysphagia (defective peristalsis / stricture) - Odynophagia (severe oesophagitis) - Haematemesis
Gastro-oesophageal reflux disease Complication Oesophageal: Oesophagitis Barrett’s (10%) Strictures Adenocarcinoma 50% of Px with GORD get complications
Gastro-oesophageal reflux disease Complication Extra-oesophageal: Laryngitis Pharyngitis Sinusitis Pulmonary Adult onset asthma NB Poor correlation between frequency and severity of symptoms and prevalence of complication
Gastro-oesophageal reflux disease GESA recommendation for Mx: Mild symptoms - Antacids /over the counter H2 antagonists - Lifestyle changes: Diet (Fatty, Spicy, Coffee, Acidic) ETOH (moderation OK) Smoking Late/large meals & early recumbency Drugs Tight clothes
Gastro-oesophageal reflux disease GESA recommendation for Mx: Moderate to severe symptoms - First line Rx: 2-4/52 of double dose PPI (Superior to endoscopy for Dx) - Symptomatic control equates to endoscopic healing (even LA Grade C&D)
Gastro-oesophageal reflux disease GESA recommendation for Mx - Further Ix if: Unclear Dx Symptoms persist/progress on Rx Complicated Symptoms Suggestion of other pathology (Ca, PUD, infective/drug induced oesphagitis)
Gastro-oesophageal reflux disease GESA recommendation for Mx - Further Ix: Endoscopy Negative in >50% of Px with GORD Ideal for: - Dx and grading of oesophagitis - Other mucosal lesions - Dx and Rx strictures - Dx of Barrett’s
Gastro-oesophageal reflux disease GESA recommendation for Mx - Further Ix: 24/24 ambulatory oesophageal pH monitoring pH <4 for >1 ½ hours
Gastro-oesophageal reflux disease GESA recommendation for Mx Trial of withdrawal of therapy Majority will have symptom relapse Repeat course of the previous Rx Followed by on demand H2 antagonist / PPI ± antacids → a small proportion will be symptom free → Majority continuous treatment / Surgery
Gastro-oesophageal reflux disease Few topics of interest - Barrett’s oesophagus - Dysplasia - H Pylori -Non-Acidreflux
Gastro-oesophageal reflux disease Barrett’s - Transformation of pseudostartified to columnar epithelium If gastric or pancreatic (rarer) → no ↑ risk of AdenoCa - Specialised intestinal metaplasia → ↑ risk of AdenoCa (much less if length <3cm) - Second yearly surveillance endoscopy with Bx (4 quadrant @ 2cm intervals) (GESA)
Gastro-oesophageal reflux disease Barrett’s - Once present → no evidence that Acid suppression will reverse progression to dysplasia - Recent study showed in Px with Barrett’s there is ↓ progression after antireflux surgery(3). - Also increased evidence in the role if Bile salts in Barrett’s(4).
Gastro-oesophageal reflux disease Non-Acid reflux(5) - Animal studies have shown: Acid alone requires high concentration to damage the oesophageal mucosa - Oesophagitis has been observed in achlorhydric patients - Duodenogastro-oesophageal reflux (DGOR) is the reflux of duodenal content (bile acids and pancreatic secretions) into the stomach (normal – postprandially and nocturnally)
Gastro-oesophageal reflux disease Non-Acid reflux(5) - Contains trypsin as well as bile acids and can occurs at neutral and acidic pH too - Conjugated Bile salts @ low pH, Unconjugated bile salts and trypsin @ high pH → can damage mucosa - Clinical studies: There is evidence that mucosal damage increase with increased exposure to the duodenogastro-oesophageal reflux.
Gastro-oesophageal reflux disease Non-Acid reflux(5) - Investigations . Scintigraphy (injection ofTc99m → @ 5 min interval →γCamera for 60/60 → can show duodenal reflux . Bilitec 2000 is spectrophometry, measure the bilirubin concentration in the oesophagus. (can have ambulatory monitoring) Problem with very low pH, food & mucosal folds
Gastro-oesophageal reflux disease Non-Acid reflux(5) - Intraluminal impedance . It measures the opposition of current flow between 2 electrodes. . Bolus movement in hollow organs. . Detects wall, air, saliva and food all vary. It is pH independent and can determine the type and height of the refluxate
Surgical Treatment of GORD - Surgery attempts to return the gastroesophageal junction below the diaphragm and form a barrier to reflux. - NB acid suppression with PPI might not be enough to prevent symptoms (impaired oesophageal clearance / non-acid reflux). - The cost of 10 year PPI treatment is ten times that of laparoscopic Nissen, including preoperative evaluation and postoperative care(7).
Surgical Treatment of GORD Hill’s posterior gastropexy - Musculomucosal flap valve created by the angle of His against the lesser curve - an important barrier to reflux. - Anchoring the LOS within the abdomen and posteriorly fixing it to the median arcuate ligament and accentuating the angle of His. - Not popular → difficulty identifying the arcuate ligament.
Surgical Treatment of GORD Hill’s posterior gastropexy - Modified Hill’s uses the preaortic fascia and the condensation of the crus as the anchor for the repair. - Good to excellent result, ? less side effect than fundoplication.
Surgical Treatment of GORD Fundoplication - Mobilise the lower oesophagus and wrap the fundus of the stomach around it either totally or partially
Surgical Treatment of GORD TotalFundoplication: - Originally described by Nissen in 1956 360° fundal wrap around the distal oesophagus with division of the short gastric vessels (“floppy”). - Modified (Rosetti & others) → not dividing the short gastrics and using a lower part of the fundus/greater curve for the wrap (no evidence for ↑dysphagia and some evidence ↓ flatulence)(8)
Surgical Treatment of GORD NissenFundoplication: - The fold should be approximately 2 cm – wider (too generous) can cause dysphagia