Download
1 / 45
500 likes | 679 Views
AVN of the Femoral Head. Jeff Easom, D.O. Garden City Hospital. Introduction. Debilitating disease that usually leads to hip joint destruction 30 to 50 year old age group (avg. 33) Ten to twenty thousand new patients annually 5 to 12% of THA annually secondary to AVN BL in 50 to 80 of pts.

E N D
AVN of the Femoral Head Jeff Easom, D.O. Garden City Hospital
Introduction • Debilitating disease that usually leads to hip joint destruction • 30 to 50 year old age group (avg. 33) • Ten to twenty thousand new patients annually • 5 to 12% of THA annually secondary to AVN • BL in 50 to 80 of pts
Etiology • Healthy cancellous bone replaced by dead trabecular bone. • Bone and marrow death can result from vascular interruption by various means and may extend to subchondral plate • Anterolateral femur predominantly affected
Presumed mechanism of mechanical failure due to accumulated stress fractures of unrepaired necrotic trabeculae • “Crescent sign” - Earliest sign of mechanical failure • No collateral vasculature in areas of subchondral bone
Clinical Conditions Assoc. with AVN • Corticosteroids(SLE, RA, renal transplant, asthma) • ETOH, Sickle Cell, Gaucher, coagulation deficiencies, myeloproliferative disorders, trauma, Caisson disease, radiation
ETOH and corticosteroids account for approx 90% of AVN (non-traumatic)-Mont et al, JBJS, Vol 77A, No. 3, March 1995 • Increased risk in individuals who drink as little as 400ml/week (JBJS, Vol 77A, No. 3, March 1995
Pathogenesis • Multiple theories • Thromboemboli, nitrogen bubbles, abnormally shaped RBC’s, ^bone marrow pressure, radiation damage, altered lipid metabolism, vasoactive factor release as Gaucher disease • AVN is multifactorial in origin with a final common pathway
Pathology • Subchondral infarcted bone>inneffective healing response>resorption of dead bone>replacement with fibrous and granulation tissue>thick trabeculae formation>cartilage collapse
Clinical Features • Severe pain over anterior hip and groin (deep or throbbing pain) • Pain worsened with WB and motion (esp. forced internal rotation) • Acute or insiduous onset • Night pain • Positive Trendelenburg sign
Diagnosis • AP/frog-leg lateral radiographs • Bone scan/bone bx- not standard diagnostic test • MRI - aids in determining extent. Earliest finding is a single density line on T1-weighted images, double-line sign on T2-weighted images
Diagnosis does not depend on a single finding, but based on the entire clinical picture, hx, and PE. • HIGH index of suspicion
Staging • Ficat and Arlet - Based on standard radiographs • Steinberg - Expanded Ficat and Arlet to include extent of femoral head involvement • Marcus • Japanese Investigation Committee - Modified Ficat and Arlet to include location of lesion
Steinberg Mild - <15% of femoral head involved Moderate – 15 to 30% Severe - >30%
ARCO(Association Research Circulation Osseous) - proposed new classification to include prior 3 classification systems. Not universally accepted or finalized yet.(JBJS,Vol 77-A, No. 3, March 1995) • Expanded Ficat and Arlet to incorporate concept of location of lesion on radiograph. • Type-A-medial, Type-B-central, and Type C-lateral
Natural History • Remains uncertain • Studies have shown that > 85% rate of collapse within 2 years when stages I and II symptomatic hips were left untreated • Overall, when the diagnosis is made, the condition will progress
Non-Operative Treatment • Observation • Protected Weight-Bearing • 21 studies/819 hips - 182(22%) with satisfactory clinical result with avg. f/u of 34 months. (Mont et al JBJS, Vol 77-A, No. 3, March 1995 • Pharmacological Tx - Limited use and studies uncontrolled
Preliminary investigation of vasoactive and lipid-lowering agents are ongoing at several centers • Electrical stimulation - Remains experimental. Mixed outcomes with published articles
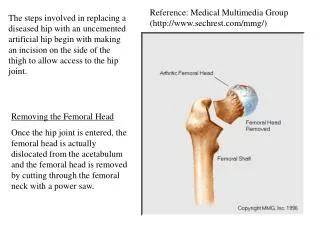
Operative Treatment • Core Decompression (with/without electrical stimulation). Stages I and II • Osteotomy(Varus, Flexion, Rotational). Stages III and IV • Non-Vascularized Bone-Grafting • Vascularized Grafts • Bipolar hemiarthroplasty, TARA, THA
Core Decompression • Stage I and II - no subchondral fracture or collapse
Mont et al, CORR, No. 324, March 1996 • 42 studies/2025 hips tx with core decompression(1206 hips) and non-operative management(819). Satisfactory results (63.5%/24 studies) of core decompression. 63% showed no evidence of radiograph disease prog. • 22.7% success/21 studies of non-operative group
84% femoral head survival with Stage I, 65% with Stage II, and 47% with Stage III in the core decompression group • 35% hip survival rates for Stage I, 31% for Stage II, and 13% for Stage III in non-operative treatment group
Stulberg et al, CORR, No. 268, July 1991 • Prospective study over 4 year period • 55 hips/36 patients • 29 core decompression/26 non-operative • Avg. age 38 • Avg. f/u 27 months
Result • Success based on HHS. Stage I - 70% (7/10 operative hips) and 20%(1/5) in non-operative hips. Stage II - 71% (5/7) and 0/7 of non-operative. Stage III - 73% (8/11) operative and 1/10 non-operative • Results of success based on HHS and not on radiographic criteria
Core and Bone Grafting - Vascularized Fibular Graft • Attempts to enhance revascularization and arrest progression of necrosis • 60 to 90% success rate • Stage II, III, IV, V - Urbaniak
Urbaniak et al, JBJS, Vol 77-A, No. 5, May 1995 • Free vascularized fibular grafting in symptomatic AVN - prospective • 103 hips/89 pts followed (median f/u 7 years • Followed yearly with regard to HHS, radiographic progression, and conversion to THA
Results • Probability of conversion to THA within 5 years was 11%(Stage II), 23%(Stage III), 43% (Stage IV), 32% (Stage V) • HHS - Improvement from 56 to 80 (Stage II), 52 to 85 (Stage III), 41 to 76 (stage IV), and 36 to 75 (Stage V). • Radiographic progression occurred in 7/19 stage II, 21/22 stage III, 31/40 stage IV, and 16/22 stage V
Osteotomy • Predicated on concept of realignment with relief of lesion from weightbearing zone (delivered from weight bearing or contained within acetabulum) • Varus, flexion, valgus-flexion, and rotational osteotomies • With lesions of a total of 200 degrees, osteotomy is not recommended
All usually require an extended period of limited weight bearing of up to a year • Sugioka et al - Transtrochanteric rotational osteotomy. Technically demanding and results have not been duplicated • Various osteotomies exist with outcomes being widely varied
Difficulty with osteotomy is the increased difficulty in obtaining a satisfactory result if a THA is necessary • 93/105 THA’s after osteotomy had intraoperative difficulties(screw removal and femoral reaming) • Ideal candidate is stage III with a small lesion and no ongoing cause of AVN
Additional Treatment Alternatives • Bipolar hemiarthroplasty - not recommended now • TARA - Older design prosthesis yielded poor results, while newer prosthetic design may yield better outcomes • Arthrodesis- Not widely advocated
Hungerford et al, JBJS, Vol 80-A, No. 11, November 1998 • 33 hips/25 pts • Ficat Stage III and early Stage IV-( collapse without involvement of acetabulum) • TARA (Depuy) • Mean f/u – 10.5 years • Mean age – 41 y.o. • Femoral head resurfacing only
Results • 30 hips/91% survived at least 5 years • Mean f/u 10.5 yrs – Overall, 20 hips(61%) had good or excellent results based on HHS;13(39%) had fair or poor result and required THA • Mean interval b/w TARA and THA – 60 months
HHS – Mean improvement from 38 points (range of 29 to 61 points) preoperatively to 91 points(range of 80 to 100.
Conclusion • After determination of whether or not collapse has occurred, one must consider the extent of the lesion, which has been found to be important prognostically(lesions involving < 15% of femoral head fare better with all treatment method than moderate or severe lesions
Medial (type-A) lesions have been found to have a much better prognosis than central (type-B), or lateral (type-C). • Overall, patients with multisystem disease or post transplantation state should have THA as a definitive procedure rather than preservation procedures
Conservative tx – 20% survival rate at 3 to 5 years for Stage I and II AVN • Core decompression – 70 to 80% survival rate in Stage I and II AVN at 3 to 5 years • Vascularized fibular grafting – Clinical success approx 70 – 80% in Stage III, IV, and V AVN
Osteotomy – 50 to 70% success rate at 5 years in Stage III AVN • THA – Higher rate of failure than for OA, but clinically better than alternatives for advanced disease • TARA – Best study represents 61% clinical success at 10.5 years