
Influence of Neighborhood Socioeconomic Status on Myocardial Infarction Treatment
This study from the ARIC examines how neighborhood income affects post-MI treatment disparities, with analyses on medication classes received and their associations with socioeconomic context.

Influence of Neighborhood Socioeconomic Status on Myocardial Infarction Treatment
E N D
Presentation Transcript
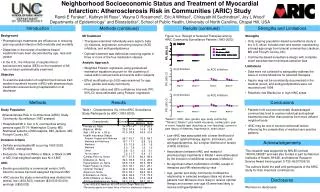
Neighborhood Socioeconomic Status and Treatment of Myocardial Infarction: Atherosclerosis Risk in Communities (ARIC) Study Randi E Foraker1, Kathryn M Rose1, Wayne D Rosamond1, Eric A Whitsel1, Chirayath M Suchindran2, Joy L Wood1 Departments of Epidemiology1 and Biostatistics2, School of Public Health, University of North Carolina, Chapel Hill, USA (b) β-blockers (b) β-blockers PR, 95% CI PR, 95% CI (c) ACE Inhibitors (c) ACE Inhibitors Introduction Methods (continued) Results (continued) Strengths and Limitations • Background • Pharmacologic treatments are efficacious in reducing post-myocardial infarction (MI) morbidity and mortality • Disparities in the receipt of evidence-based treatments have been documented by age, race and gender • In the U.S., the influence of neighborhood socioeconomic status (SES) on the treatment of MI has not been systematically examined • Objective • To examine association of neighborhood census tract median household income (nINC) with pharmacologic treatments received during hospitalization or at discharge • MI Treatment • Therapies examined individually were aspirin, beta ()-blockers, angiotensin converting enzyme (ACE) inhibitors, and antihyperlipidemics • Optimal treatment was defined as receiving agents in three or more of the four medication classes • Analytic Approach • Weighted Poisson regression using generalized estimation equations account for the clustering of cases within census tracts and events within subjects • Effect modification (p<0.05) was examined for age, race, gender and study community • Prevalence ratios and 95% confidence intervals (PR, 95% CI) were estimated using Poisson regression Figure 1a-e. Receipt of Selected Therapies among ARIC Community Surveillance Patients (1993-2002) *Model 1: nINC, race, gender, age, study community**Model 2: Model 1 plus health insurance, cardiac pain, year of event, hospital type (teaching vs. non-teaching); current or past history of diabetes, hypertension, heart failure • Strengths • Only ongoing population-based surveillance study in the U.S. which includes men and women representing a broad age range from biracial communities (Jackson, MS and Forsyth County, NC) • Community-based surveillance design with complete event ascertainment minimizes selection bias • Limitations • Data were not collected to adequately address the issue of contraindications for selected therapies • Aspirin may not be consistently documented in the medical record, and antihyperlipidemics were not recorded until 1998 • Relatively few Blacks live in high nINC areas Methods Results Conclusions • Study Population • Atherosclerosis Risk in Communities (ARIC) Study Community Surveillance (1987-present) • Hospitalized MI in four U.S. communities among persons aged 35-74: Washington County, MD; Northwest suburbs of Minneapolis, MN; Jackson, MS; Forsyth County, NC • Inclusion Criteria • Definite and probable MI occurring 1993-2002 (N=9560, unweighted) • Exclusions: Race not White or Black, or Black in MN or MD; final weighted sample size N=13,805 • nINC • Events geocoded by a commercial vendor; 94% linked to census tract and assigned tract-level nINC • nINC across the study communities was divided into tertiles: low (<$33,533), medium ($33,533-50,031) and high (≥$50,032) Table 1. Characteristics (%) of the ARIC Surveillance Study Participants by nINC (1993-2002) • Patients from socioeconomically disadvantaged communities tend to receive individual and optimal treatments less often than patients from more affluent neighborhoods • nINC may be one of several contextual factors influencing the complexities of medical care practice patterns • Low nINC was associated with a lower likelihood of receipt of optimal therapy, aspirin, β-blockers, and antihyperlipidemics, but a higher likelihood of receipt of ACE inhibitors • Associations between nINC and receipt of pharmacologic treatments in Model 1 were attenuated by the inclusion of additional covariates in Model 2 • No significant effect modification of nINC-receipt of therapies post-MI relationship by race • Age, gender and study community modified the relationship in selected analyses (data not shown): patients from MN were more likely to receive optimal therapy and women over age 65 were less likely to receive antihyperlipidemics Acknowledgements This research was supported by NHLBI contract 1R01HL080287 and was also funded in part by National Institutes of Health, NHLBI, and National Research Service Award training grant 5-T32-HL007055-30. The authors thank the staff and participants of the ARIC study for their important contributions. Disclosures We have no disclosures





