Download
1 / 65
720 likes | 845 Views
Explore the characteristics, etiological factors, and pathogenesis of restrictive lung diseases, including Acute Respiratory Distress Syndrome (ARDS) and Hypersensitivity Pneumonitis. Learn about the phases of ARDS, its mortality rates, and important causes. Dive into the pathology of diffuse alveolar damage, fibrosis, and interstitial lung diseases.

E N D
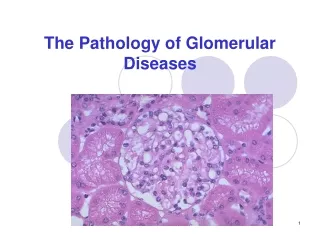
The Pathology of Lung Diseases I. RESTRICTIVE LUNG DISEASES II. OBSTRUCTIVE LUNG DISEASES
I.RESTRICTIVE LUNG DISEASES-Diffuse Interstitial Lung Disease-InfiltrativeLung Disease-Fibrosing alveolitis-Honeycomb lung
Restrictive lung diseases are characterized by reduced lung volume, an alteration in lung parenchyma a disease of the pleura or chest wall a disease of neuromuscular apparatus In physiological terms, restrictive lung diseases are characterized by reduced lung capacity; reduced total lung capacity (TLC) reduced vital capacity reduced resting lung volume
The many disorders that cause reduction or restriction of lung volumes may be divided into 2 groups based on anatomical structures: 1. Intrinsic lung diseases (or diseases of the lung parenchyma), 2.Extrinsic disorders (or extraparenchymal diseases).
1. Intrinsic lung diseases or diseases of the lung parenchyma: The diseases cause inflammation or scarring of the lung tissue (interstitial lung disease) or result in filling of the air spaces with exudate and debris (pneumonitis).
2. Extrinsic disorders or extraparenchymal diseases: Nonmuscular diseases of the chest wall, and neuromuscular disorders The chest wall, pleura, and respiratory muscles are the components of the respiratory pump, and they need to function normally for effective ventilation. If not; impaired ventilatory function, respiratory failure.
Intrinsic lung diseases or Diseases of the lung parenchyma RESTRICTIVE LUNG DISEASES
These diseases can be characterized according to etiological factors: • Acute restrictive pulmonary diseases (acute lung injury) • Acute Respiratory Distress Syndrome (ARDS) • Acute Hypersensitivity Pneumonitis • Chronic restrictive pulmonary diseases • Idiopathic fibrotic diseases • Connective tissue diseases • Drug-induced lung disease • Primary diseases of the lungs (including sarcoidosis)
Acute Lung Injury 1. Diffuse Alveolar Damage (Acute Respiratory Distress Syndrome - ARDS) 2. Acute Hypersensitivity Pneumonitis (Extrinsic Allergic Alveolitis)
1. Diffuse Alveolar Damage (Acute Respiratory Distress Syndrome - ARDS) • Diffuse alveolar damage (DAD) refers to a pattern of reaction to injury of alveolar epithelial and endothelial cells from a variety of acute insults. • The clinical counterpart of severe DAD is the acute respiratory distress syndrome (ARDS). • In this disorder, a patient with apparently normal lungs sustains pulmonary damage and then develops rapidly progressive respiratory failure. • The condition reflects decreased lung compliance (usually requiring mechanical ventilation) and hypoxemia and features extensive radiologic opacities in both lungs (white-out). • The overall mortality of ARDS is more than 50%, and in patients older than 60 years, it is as high as 90%.
ETIOLOGY: Important Causes of the Acute Respiratory Distress Syndrome
Acute Respiratory Distress Syndrome: Pathogenesis Endothelial/capillary injury alveolar capillary membrane damage increased vascular permeability edema (interstitial/alveolar) increased synthesis of neutrophil chemotacatic & activating agents (IL) activated neutrophils oxidants, proteases, PAF, leukotriens tissue damage other mediators stimulating collagen production Fibrosis
Pathology Exudative phase (0-7 days): congestion, necrosis of alveolar epithelial cells, edema, hemorrhage, neutrophils in capillaries, Destruction of type I pneumocytes permits exudation of fluid into alveolar spaces, where deposition of plasma proteins results in formation of fibrin-containing precipitates(hyaline membranes)on the injured alveolar walls
congestion • necrosis of alveolar epithelial cells • edema • hemorrhage • neutrophils in capillaries • hyaline membranes
If the patient survives the acute phase of ARDS Proliferative phase (1-3 weeks): Proliferation of type II pneumocytes Cleaning of remnant hyaline membranes by pulmonary macrophages Expansion of alveolar septa Proliferation of fibroblasts Collagen tissue production Healing or Fibrosing Fibrosing phase: Diffuse interstitial fibrosis Honeycomb lung
Proliferation of type II pneumocytes • Cleaning of remnant hyaline membranes by pulmonary macrophages • Expansion of alveolar septa • Proliferation of fibroblasts
Diffuse interstitial fibrosis • Honeycomb lung.
2. Acute Hypersensitivity Pneumonitis (Extrinsic Allergic Alveolitis) • A response to inhaled antigens • Farmer's lung occurs in farmers exposed to Micropolyspora faeni from moldy hay • Bagassosis results from exposure to Thermoactinomyces sacchari in moldy sugar cane • Maple bark-stripper's disease is seen in persons exposed to the fungus Cryptostroma corticale from moldy maple bark • Bird fancier's lung affects bird keepers with long-term exposure to proteins from bird feathers, blood and excrement • Hypersensitivity pneumonitis may also be caused by fungi growing in stagnant water in air conditioners, swimming pools, hot tubs, and central heating units. • Skin tests and serum precipitating antibodies are often used to confirm the diagnosis. • In many cases, especially in the chronic form of hypersensitivity pneumonitis, the inciting antigen is never identified.
CHRONIC INTERSTITIAL LUNG DISEASES Characterized by - decreased lung volume - decreased oxygen-diffusing capacity on pulmonary function studies
A large number of pulmonary disorders are grouped as interstitial, infiltrative, or restrictive diseases • They are characterized by inflammatory infiltrates in the interstitial space and have similar clinical and radiologic presentations • These diverse maladies (1) are of known or unknown etiology, and (2) vary from minimally symptomatic conditions to severely incapacitating and lethal interstitial fibrosis
Etiology • Occupational/environmental diseases (24%) • Sarcoidosis (20%) • Idiopathic pulmonary fibrosis (15%) • Collagen-vascular diseases (8%) The remainder have more than 100 different causes and associations.
The most striking findings are; Longstanding inflammatory damage Fibrosis of the alveolar walls Fibrosis finally wipes out groups of alveoli Scar contraction of respiratory bronchioles The radiographic and autopsy diagnosis of "honeycomb lung"
ORGANIC DUST EXPOSURE • Chronic Hypersensitivity Pneumonitis • Chronic form of Acute Hypersensitivity Pneumonitis • The prototype of hypersensitivity pneumonitis is farmer's lung • Cause: Inhalation of thermophilic actinomycetes that grow in moldy hay • Patients with the chronic form of hypersensitivity pneumonitis have a more nonspecific presentation, with indolent onset of dyspnea and cor pulmonale.
Pathology: • The main microscopic features of chronic hypersensitivity pneumonitis include • bronchiolocentric cellular interstitial pneumonia • noncaseating granulomas (in two thirds of cases) • organizing pneumonia • The bronchiolocentric cellular interstitial infiltrate • lymphocytes • plasma cells • macrophages
Patchy mononuclear cell infiltrates, • Lymphocytes • Plasma cells • Epitheloid histiocytes • Interstitial noncaseating granulomas, • Interstitial fibrosis.
INORGANIC DUST EXPOSURE • Pneumoconioses • Dust inhalation • Silicosis • Asbestosis • Talcosis • Historically, knife grinder's lung (silicosis).
Mineral dust-induced lung diseases • Coal dust (upper lobe) • Silica (upper lobe) • Asbestos (lower lobe) • Beryllium : Coal workers : Stone, Ceramics, Sandblasting : Mining, Milling, Insulation : Nuclear energy, Aircraft industry
Particles over 10 µm in diameter deposit on bronchi and bronchioles and are removed by the mucociliary escalator. • Smaller particles reach the acinus, and the smallest ones behave as a gas and are exhaled. • Alveolar macrophages ingest the inhaled particles and are the primary defenders of the alveolar space. • Most phagocytosed particles ascend to the mucociliary carpet and are expectorated or swallowed. • Others migrate into the interstitium of the lung, then into the lymphatics.
Air particulate exposure • Pneumoconioses • Pulmonary fibrosis • Asthma • Chronic bronchitis • Lung cancer
INORGANIC DUST EXPOSURE: Silicosis • Inhalation of silicon dioxide (silica) • History: Dyspnea in metal diggers was reported by Hippocrates • Early Dutch pathologists wrote that the lungs of stone cutters sectioned like a mass of sand. • The major cause of death in workers exposed to silica dust for the first half of the 20th century • Sandblasters • Stone cutting • Polishing and sharpening of metals • Ceramic manufacturing • Foundry work
After their inhalation, silica particles are ingested by alveolar macrophages • Silicon hydroxide groups on the surface of the particles form hydrogen bonds with phospholipids and proteins, an interaction that is presumed to damage cellular membranes and thereby kill the macrophages • The dead cells release free silica particles and fibrogenic factors progressive massive fibrosis • The released silica is then reingested by macrophages and the process is amplified
The nodular lesions consist of concentric layers of hyalinized collagen • Surrounded by a dense capsule of more condensed collagen • Examination of the nodules by polarized microscopy reveals the birefringent silica particles.
INORGANIC DUST EXPOSURE:Coal Workers' Pneumoconiosis (CWP) • Coal dust is composed of amorphous carbon and other constituents of the earth's surface, including variable amounts of silica. • Anthracite (hard) coal contains significantly more quartz • Amorphous carbon by itself is not fibrogenic • Silica is highly fibrogenic, and inhaled anthracotic particles may thus lead to anthracosilicosis.
Asymptomatic anthracosis • Simple CWP: • Coal macules • Coal nodules • Complicated CWP • Caplan syndrome
CWP • Simple CWP • Complicated CWP (progressive massive fibrosis) • Coal-dust macules and coal-dust nodules: • Both are typically multiple and scattered throughout the lung as 1- to 4-mm black foci • Microscopy • Coal-dust macule: numerous carbon-laden macrophages • Coal-dust nodule: round or irregular; dust-laden macrophages associated + fibrotic stroma • Focal dust emphysema
Coal workers’ pneumoconiosis (CWP) Coal-dust nodule + Focal dust emphysema
Caplan syndrome • Rheumatoid nodules (Caplan nodules) in the lungs of coal miners with rheumatoid arthritis. • Nodular lesions (1-10 cm in diameter) • Multiple, bilateral, and usually peripheral • Microscopy • Rheumatoid nodule + dust deposits • Rheumatoid nodules consist of large, central, necrotic areas surrounded by a border of chronic inflammation and palisading macrophages.
INORGANIC DUST EXPOSURE: Asbestosis • Asbestos - a group of fibrous silicate minerals • Insulation • Construction materials • Automative brake linings
Asbestos is a naturally occurring fibrous silicate that was widely used in the past for commercial applications because of its heat-resistance properties. • Geometric forms of asbestos: • 1. Amphibole (straight, stiff, and brittle fibers). • 2. Serpentine (curly and flexible fibers; 90% used in wide-world).
Asbestos exposure has been industrial or occupational and primarily affects workers involved in: • mining or processing asbestos • shipbuilding • construction • textile • insulation-manufacturing industries • However, because the latency period between an initial exposure and the development of most asbestos-related disease is 20 years or longer, • Asbestos-related disease remains an important public health issue.
Exposure to asbestos can cause a number of thoracic complications • Asbestosis • Benign pleural effusion • Pleural plaques • Diffuse pleural fibrosis • Rounded atelectasis • Mesothelioma • Lung carcinoma
ASBESTOSIS • Asbestosis is diffuse interstitial fibrosis resulting from inhalation of asbestos fibers • The development of asbestosis requires heavy exposure to asbestos • Asbestos may produce obstructive as well as restrictive defects • As the disease progresses, fibrosis spreads beyond the peribronchiolar location and eventually results in an end-stage or (honeycomb) lung • Asbestosis is usually more severe in the lower zones of the lung
Pathology • Lower lobes and subpleural • Diffuse pulmonary interstitial fibrosis • Asbestos bodies(golden brown, fusiform or beaded rods with a translucent center and knobbod ends) • Asbestos fibers coated with an iron-containing proteinaceous material(ferruginous body)
Lower lobes and subpleural • Diffuse pulmonary interstitial fibrosis
Asbestos fibers coated with an iron-containing proteinaceous material (ferruginous body)