Download
1 / 42
420 likes | 518 Views
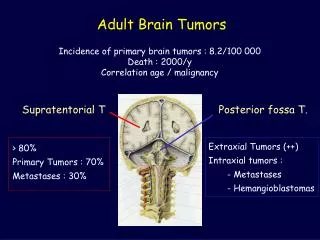
BRAIN TUMORS : Epidemiology:82/100000 20% of malignancies of<15 years Incidence peak in childhood increase from20 to70 years decease >70 Glioma M>F Meningioma F>M. In childhood:Medulloblastoma& Astrocytoma In adults:Glioma&Meningioma In childhhod:70% infratentorial

E N D
BRAIN TUMORS: Epidemiology:82/100000 20% of malignancies of<15 years Incidence peak in childhood increase from20 to70 years decease>70 Glioma M>F Meningioma F>M
In childhood:Medulloblastoma& Astrocytoma In adults:Glioma&Meningioma In childhhod:70% infratentorial In adult:70% supratentorial Survival in children is better
Riskfactors: stroke,menopose,breast cancer,farmacotics EBV CNS lymphoma JCV PML Astrocytoma Radiation Antioxidants--------preventive
Clinical Diagnosis: Mass effect-Edema-IICP Negative &Positive Signs Headache Vomiting Facial pain
Seizure(30-70%)-focal Changes of conciousness(frontal) Frontal SOL:silent-personalitydisorder Abulia-Judjment dis-incontinency- Primitive reflexes OcciputalSOL:Visual field changes
TemporalSOL: Seizure-Aphasia- Visual field disturbance ParietalSOL: Cortical sensoryloss Neglect-Anosognosis- Hemiparesis-Visuospatial D Thalamic SOL: Hemisensoryloss
Brain stem SOL: Cranial nerve palsy Hicough-Vomiting-Hemiparesis Pineal SOL: Parinaud syn.-Premature Puberty-Hydrocephalus Cerebellar SOL; Headache-Vomiting Neck stiffness-Ataxia
Acoustic neuroma; Deafness-Facial weakness-vertigo Pituitary adenoma: Bitemporal hemianopia Neuroophthalmologic signs: Parinaud syn.-Ptosis-papiledema- Optic atrophy-Foster kennedy syn.
Laboratory Findings: Skull x ray-Brain CT scan&MRI- Angiography-MRA-PET&SPECT Evoked potentials-EEG D.D: Stoke-Infection-MS-Sarcoidosis
meningiomas: F>M-6th&7th decade- childhood(rarely)-90% intracranial Ethiology; Radiation-Trauma?- progestrone-Viral Clinical Manifestations: Seizure- Hemiparesis-cranial palsy-IICP
Imaging:x ray-CT-MRI-MRA Treatment:Resection-Radiothrapy- Proton beam- Mifepristone(RU486 -Chemothrapy(Ifosfamide)-AEDs Gliomas:60%primary brain tumors low grade- high grade
<25 years67% infratentorial >25years 90% supratentorial Location: white matter (frontal-temporal-frontoparietal) Symptoms: Seizure-focal deficits- Memmory& personality disturbance Treatment: Resection-radiation-chemotherapy (carmustin& procarbazin)
Oligodendroglioma: Sensitive to chemothrapy-5% SOL-50YEARS Symptoms: Seizure-focal deficit Imaging: Hypodensity-calcification Treatment: Resection –Radiation- Chemothrapy(PCV-CCNU)
Ependymoma:3-5years-vomiting Hydrocephalus Location: Ventricles-spinal cord Treatment: Resection-Radiation PNET: Childhood-Mitosis-Invasive Medulloblastoma: Vermis Treatment: Mixed thrapy
; Brain Metastasis The most common direct neurological complication of Systemic cancer BM>primary malignant brain tumor 10 times Prostate cancer 1%BM ovarian cancer 3% BM Melanoma 18-90%BM lung cancer 18-63%
; Breast cancer 20-30%BM 20-40% dying with cancer have BM BM causes :lung(40-50%)-breast(15-20%)-melanoma& GI and renal (every one 5-10
; BM 80% supratentorial Pelvic &GI cancer infratentorial Initial manifestation of unknown systemic tumor 10-30% Lung cancer:the most common cause of BM presentig Without a known primary (66%) NSCLC –GI(10%) Intratumoral hemorrhage; melanoma-choriocarcinoma- thyroid &renal cell carcinoma
; Clinical presentation may arise as long as 20 years after discovery of the primary tumor (breast-melanoma) may antedate discovery primary tumor (lung) progressive over days or weeks (occasionally acute seizure or stroke like) Headache 50%-mental status changes 33% tension like –classic brain tumor headache is uncommon
; Headache without other symptoms compatible With multiple metastasis Nausea- vomiting-drowsiness- unilateral weakness- gait disturbance- seizure Signs :hemiparesis &mental status changes (the most common 60%)- IICP- pappiledema(10%)
; D D :primary SOL-abcess- MS- stroke PML- radiation therapy Neuroimaging:T2 MRI detect >1cm diameter MRI with gadolinium improved sensivity multiple metastasis (70-75%)
Pituitary tumors:2/7-27% M=F 3&4 DECADE-Sporadic-10% inchildhood Secratory&Nonsecratory Prolactinoma; Most common Mixed: 10% Microadenoma---Macroadenoma
Pituitary tumors:2/7-27% M=F 3&4 DECADE-Sporadic-10% inchildhood Secratory&Nonsecratory Prolactinoma; Most common Mixed: 10% Microadenoma---Macroadenoma
Adenocarcinoma:Rarely Clinical Manifestations: Mass effect(headache&visual loss &hypopituitarism)-papilledema(rare Dysfunction of ocular nerves-IICP -DI-Seizure-hemiparesis-dementia
Management: Evaluation of endocrine-thyroid& adrenal replacement-Bromocriptin -Resection-Radiothrapy Pituitary apoplexy: sever headache-vomiting-nausea ;
; SPINAL TUMORS : Divided by location : 1)intramedullary 2)intradural 3)extradural intramedullary are rare 10% intradural” menengioma-neurofibroma benign encapsulated 65% IM more common in childhood EM are more common in adults The most common primary sites of metastasis :a)lung b) breast c)prostate d)GI,lymphoma,melanoma,renal,….
; M=F SPINAL/BRAIN= 25% meningioma F>M ependymoma M>F Spinal tumors occur prodominant in young or middle aged and are less common in childhood or after age 60 years most often ln thoracic region
; Symptoms : Intradural : compression nerve roots-(dorsal)-ultimately complete loss of function below the level of the lesion 1)focal pain &paresthesias 2) sensory loss weakness,wasting 3)cord compression(spastic weak impairment of sensation-impaired control of bladder and rectum
; Symptoms continued: overactive DTR –Babinsky sign loss of superficial abdominal reflex Spinal Metastasis :5-10%of all cancer patients Epidural spinal cord compression treatment of cord compression does not prolong survival but may relieve pain and prevent disability
; Neck or back pain persists when the patient lies in bed even if the pain relieved by analgesics. Limb weakness –paresthiasis in the distribution of nerve root- or bladder dysfunction Rarely the only manifestation of cord compression is a gait disorder (sensory ataxia or spinocerbellar)
; Lung-breast-GI-prostate-melanoma =>80% of original site Treatment is palliative Loss of bladder or bowel is an Ominous prognostic sign and is Usually irreversible Radiotherapy is treatment of Choice melanoma_surgical T
; Intramedullary metastasis: The most common sites :lung or breast 60% multiple metastasis Death 3 months of diagnosis 80% Primary intramedullary tumors: usually extend over many segments- if restricted to 1-2 the syndrome is similar to that of an extramedullary tumor sacral sparing- syringimyelia
; Intradural tumors neurofibroma: the most common meningioma- schwannoma