Urinary Tract Obstruction Classification
310 likes | 495 Views
Explore the causes, levels, and duration of urinary tract obstructions, including congenital anomalies, acquired conditions, and stages of compensation and decompensation. Learn about the pathophysiology and hemodynamic changes associated with UTO.

Urinary Tract Obstruction Classification
E N D
Presentation Transcript
Classification • according to the : • ~cause (congenital or acquired) • ~duration (acute or chronic) • ~degree (partial or complete) • ~level (upper or lower urinary tract) • .
According to cause A-congenital anomalies more common in the U.T than any other organ system. (generally obstructive) *the common sites of cong. narrowing - meatal stenosis ,posterior urethral valve -ectopic ureters, uretrocele,and the ureterovesical & ureteropelvic junctions ~Damage to the sacral roots 2-4 (spina bifida & meningomyelocele) ~vesicoureteral reflux cause both vesical & renal stasis.
B-Acquired causes numerous & primary or secondary 1-urethral stricture 2-BPH or ca of the prostate 3-vesical tumor 4-local extension of ca. of the prostate or cx. 5-ureteral stones 6-retroperitoneal fibroses or malignant tumor. 7-pregnancy. ~neurogenic dysfuncton –ureterovesical obstruction or reflux. ~sever constipation sp. In children.
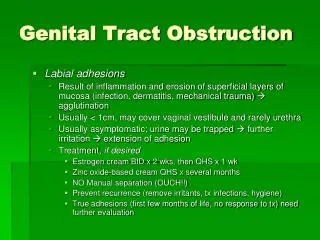
According to the level • A-lower tract(urethral stricture) • Ieading to : • dilation of the urethra. • The wall of the urethra may become thin • diverticulum may form. • periurethral abscess can result.
B- mid tract(BPH) Stage of compensation: hypertrophy of detrusorms. to overcome the urethral resistance. Complete emptying of the urinary bladder is possible. *In cystocope, autopsy or surgery we find A-Trabeculation of the bladder wall B-cellules normal intravesical pressure 30cm water at the beginning of micturition. 2-3 times as great may be reached by trabeculated this pressure tend to push mucosa between the superficial ms. bundles, causing the formation of small pockets (cellules) .
C- diverticula. ~diverticula have no ms. wall –unable to expel their content into the bl. efficiently even after obstruction removed. Stage of decompensation The compensatory power of the bladder musculature varies greatly. One patient with huge prostatic may have only mild symptoms of another may suffer acute retention and yet have a gland of normal size In the face of progressive outlet obstruction, possibly aggravated by prostatic infection with edema decompensation of the detrusor may occur
C- Upper tract Ureter in early (compensation) & reflux late (decompensation) –ureteral dilatation & hydronephrosis ~Elongation & tortuosity of ureteral ms.
Kidney pressure in the renal pelvis normally close to zero. If its increase (obstruction or reflux) –dilatation of the pelvis & calyces (hydronephrosis) which depend on duration, degree & site of obstruction. -the higher the obstruction the greater effect on the kidney. -intrarenal pelvis all the pressure exerted on parenchyma, while only part of the pressure in extrarenal pelvis. -the pelvic ms. Also have compensation & decompensation phases.
Hydronephrotic changes; 1-the earliest changes in the calyces the papilla become flattened, then convex (clubbed). -the parenchyma; compression atrophy from increase intrapelvic pressure & ischemic atrophy pressure on arcuate artery. 2-only in unilateral hydronephrosis advance stage of hydronephrotic atrophy seen. Unlike other secretory organs (which cease secreting when their duct obstructed) the completely obstructed kidney continue to secret urine
-fluid &soluble substance reabsorbed from the pelvis through the tubule ,lymphatic or venous . -as unilateral hydronephrosis progress the normal kidney undergo compensatory hypertrophy.
Pathophysiology of urinary tract obstruction
GFR influenced by -renal plasma flow and the resistances of the afferent and efferent arterioles -The hydraulic pressure driving fluid into Bowman's space is resisted by the hydraulic pressure of fluid in the tubule -the increasing oncotic pressure of the proteins remaining in higher concentration in the late glomerular capillary
Hemodynamic Changes A number of vasoactive substances are thought to play a role in the changes in RBF and GFR occurring with both UUO & BUO *With UUO, 1-RBF increases during the first 1 to 2 hours and is accompanied by a high tubular pressure and collecting system pressure because of the obstruction
2-In a second phase lasting 3 to 4 hours, these pressure parameters remain elevated but RBF begins to decline 3-A third phase beginning about 5 hours after obstruction is characterized by a further decline in RBF, now paralleled by a decrease in tubular pressureand collecting system pressure These changes are explained by physical alterations in flow dynamics within the kidney and are modified by changes in the biochemical and hormonal milieu regulating renal resistance
-increase in tubular pressure would counterbalanced by an increase in RBF related to afferent arteriolar vasodilation, its likely that both PGE2 and NO contribute to the net renal vasodilation that occurs early following UUO -the vasodilation effect of the PGE2could be blocked by NSAIDs, a prostaglandin synthesis inhibitor
*with BUO The changes with BUO or obstruction of a solitary kidney are different In contrast to the early robust renal vasodilation with UUO, there is a modest increase in RBF with BUO lasting approximately 90 minutes followed by a prolonged and profound decrease in RBF that is greater than that found with UUO *Although in both cases ureteral and tubular pressure is increased for the first 4 to 5 hours, the ureteral pressure remains elevated for at least 24 hours with BUO
This difference between the two pathophysiologic conditions has been hypothesized to be due to an accumulation of vasoactive substances in BUO that could contribute to preglomerular vasodilation and postglomerular vasoconstriction. Such substances would not accumulate in UUO as they would be excreted by the contralateral kidney. Atrial natriuretic peptide (ANP) appears to be one of these substances
Urinary tract obstruction leads to progressive and eventually permanent changes in the structure of the kidney including the development of tubulointerstitial fibrosis, tubular atrophy and apoptosis, and interstitial inflammation
Management of urinary tract obstruction
Clinical feature A-symptom; 1-Lower & mid tract (urethra &bladder) (Urethral stricture, BPH, neurogenic bl., ca bl,) The principle symptom are -hesitancy, weak stream &terminal dribbling. -hematuria in BPH & ca bladder -burning micturition &cloudy urine if there is infection. -Occasionally urine retention.
Upper tract (ureters & kidneys) Ureteral strictures or stone & renal stone -Pain in the flank radiating along the course of the ureter, -gross total hematuria (stone) -GIT symptom, -chills, fever, burning micturition & cloudy urine (infection). -Nausea. vomiting, loss of weight & strength due to uremia (bilat. hydronephroses) .
Signs. A-lower &mid tract -induration in the urethra -DRE atony of anal sphincter, benign or malig. enlargement of the prostate. -Distended bladder by suprapubic exam. -Observation of urinary stream afford rough estimate of max. flow rate, accurately measured by flowmeter. N 20-25 ml/sec in m. & 25-30 in f. ~A flow rate under 10ml/sec. indicate either obstruction or weak detrusor function.
B- Upper tract Enlarge kidney may be discovered by palpation or percussion. Renal tenderness. Large pelvic mass (tumor, pregnancy). Laboratory finding. -microscopic hematuria -Anemia, secondary to ch. infection or renal f. -Leukocytosis -urea-creatinine ratio well above the normal 10:1. (urea is significantly reabsorbed but creatinine is not)
Diagnostic Imaging ultrasonography Safe ,non invasive, cheep, available Plain film– calcified body suggest renal or ureteric stone metastasis in the spine Excretory urograms (EXU) Limited in those who are at higher risk for developing contrast-induced nephropathy, or those with history of contrast allergy
Retrograde cystography. Trabeculation, diverticula, BPH, ca bladder, reflux. CT & MRI CT is the most accurate radiologic study for the diagnosis of ureteral calculi -all urinary calculi can be demonstrated in CT even the radiolucent in KUB film except indinavir stone
Instrumental exam. Passage of catheter– stricture, or estimate residual urine. Cystoscopic inspection of urethra &bladder may reveal the primary cause, retrograde ureteropyelograms may be obtained
Complications Stagnation– infection difficult to eradicate. urea splitting organism (proteus, staph.) cause alkaline urine –stone formation. Pyonephrosis –severely infected & obstructed Treatment A-relief of obstruction: (stone, tumor, stricture) catheterization, nephrostomy, ureterostomy or surgery. B-eradication of infection. Progx.depend on cause, site, degree, & duration of obstruction. If renal function good obstruction released, infection treated (excellent)