Download
1 / 26
310 likes | 417 Views
Learn about acid-base balance and blood gas homeostasis, crucial in assessing life-threatening conditions. Explore mechanisms to maintain balance, definitions of acid, base, buffer, and the role of strong acids and bases. Understand maintenance of hydrogen ions and regulation systems involving buffers, respiratory, and kidneys. Discover how lungs and kidneys regulate pH, the interrelationship of bicarbonate and hemoglobin systems, and the impact of ventilation on blood pH. Gain insights into the role of kidneys in selectively reabsorbing ions to maintain balance.

E N D
Blood Gases, pH and Buffer system Part 1 Lecture 16
Introduction • An important aspect of clinical chemistry is information on a patient's acid-base balance and blood gas homeostasis. • These data often are used to assess patients in life-threatening situations. • This lecture discusses: • the body's mechanisms to maintain acid-base balance and • exchange of gases, carbon dioxide and oxygen,
Definitions: Acid, Base, Buffer • Acid: • asubstance that yields H+ ions in H2O. • Base: • asubstance that yields a hydroxyl ion (OH-). • Buffer: • the combination of a weak acid and its salt, is a system that resists changes in pH.
Strong acids vs. Strong Base • Strong acids: • have pK value of less than 3.0 • Strong base: • have a pK value greater than 9.0
Acid-Base balance Maintenance of hydrogen ions: • Body produces 40-80 mmol of H/day, • normal concentration of H in ECF ranges from 36-44 nmol (pH, 7.34-7.44) • Any deviation from the values the body will try to compensate. • >44 nmol/L: altered consciousness, coma- death • <36 nmol/L: neuromuscular irritability, tetany, loss of consciousness- death.
Acid-Base balance C= concentration • Because pH is the negative log of the cH+ • Decrease in H+ ion Increase pH • Increase H + ions Decrease pH • Arterial blood pH is controlled by: • Buffers • Respiratory System • and Kidneys
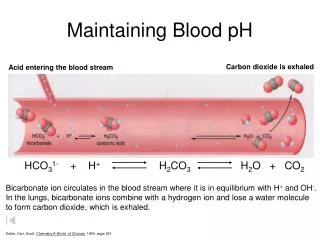
Buffer System: Regulation of H+ • First line of defense to changes in H+ consist of: • weak acid (H2CO3)& its salt (HCO3-) • Add acid to H2CO3& HCO3- system: • the HCO3- combines with H from the acid to form H2CO3. • Add a base to the system: • H2CO3 combines with OH to form H2O and HCO3 • Keeps the body at the correct pH (7.35-7.45)
Buffer System: Regulation of H+ • Bicarbonate – carbonic acid system has low buffering capacity but still an important buffer system for 3 reasons: • H2CO3 dissociates into CO2 & H2O allowing H+ to be eliminated as CO2 by lungs • Changes in CO2 modify the ventilation rate • HCO3- conc. can be altered by the kidneys
Other systems HPO4–2 H2PO4– system Proteins are capable of binding H+ Hemoglobin
Regulation of Acid-Base Balance: Lungs and Kidneys • The lungs and kidneys play important roles in regulating blood pH. • The lungs regulate pH through retention or elimination of CO2 • by changing the rate and volume of ventilation. • The kidneys regulate pH by: • excreting acid, primarily in the ammonium ion, • and by reclaiming HCO3- from the glomerular filtrate.
Regulation of Acid-Base Balance by Lungs • End product of aerobic metabolic process is CO2 • diffuses out the tissue into plasma and RBC • In Plasma & RBCs: • a small amount of CO2 is dissolved • or combined with proteins to form carbamino compounds. • Most of the CO2 combines with H2O to form H2CO3, which quickly dissociates into H+ and HCO3- • The dissociation of H2CO3 causes the HCO3- concentration to increase in the RBCs and diffuse into the plasma. • To maintain electroneutrality chloride diffuses into the cell (chloride shift)
Regulation of Acid-Base Balance by Lungs In the lungs: • The process is reversed. • Inspired O2 diffuses from the alveoli into the blood and is bound to hemoglobin, forming oxyhemoglobin (O2Hb). • The H+ that was carried on the (reduced) hemoglobin in the venous blood is released to recombine with HCO3- to form H2CO3, • which dissociates into H2O and CO2.
Regulation of Acid-Base Balance by Lungs • The CO2 diffuses into the alveoli and is eliminated through ventilation. • The net effect of the interaction of these two buffering systems is a minimal change in H+ concentration between the venous and arterial circulation.
Interrelationship of the bicarbonate and hemoglobin buffering systems
Regulation of Acid-Base Balance by Lungs • When the lungs do not remove CO2 at the rate of its production (hypoventilation) it accumulates in the blood, • causing an increase in H+ concentration. • If, however, CO2 removal is faster than production (hyperventilation) • the H+ concentration will be decreased. • Consequently, ventilation affects the pH of the blood.
Regulation of Acid-Base Balance by Lungs • A change in the H+ concentration of blood that results from nonrespiratory disturbances causes the respiratory center to respond • altering the rate of ventilation in an effort to restore the blood pH to normal. • The lungs, by responding within seconds, together with the buffer systems, provide the first line of defense to changes in acid-base status.
Kidney system • Main role is reabsorption of bicarbonate • Kidneys respond to increase or decrease in hydrogen ions by selectively excreting or reabsorbing: • Hydrogen ions • Sodium • Chloride • Phosphate • Ammonia • Bicarbonate
Reabsorption of Bicarbonate Reabsorption of bicarbonate (HCO3 –) takes place in the renal tubule cells. Na + is exchanged for H+ ion. H+ ion combines with the HCO3 – and carbonic acid dissociates into H2O and CO2. CO2 diffuses into the tubule cells combining with H2O forming H2CO3. Reabsorption of bicarbonate in the blood system. Urinary H+ combines with HPO4– and NH3.
Acid-Base Disorders Acidosis (decrease pH) → acidemia Alkalosis (increased pH) → alkalemia metabolic or respiratory A disorder caused by ventilatory dysfunction is termed primary respiratory acidosis or alkalosis. A disorder resulting from a change in the bicarbonate level is termed a nonrespiratory disorder.
Acid-Base Disorders • Body's cellular and metabolic activities are pH dependent • The body tries to restore acid-base homeostasis whenever an imbalance occurs. • This action is termed compensation • Done by altering the factor not primarily affected by the pathologic process. • eg., if the imbalance is of nonrespiratory origin, the body compensates by altering ventilation. • For disturbances of the respiratory component, the kidneys compensate by selectively excreting or reabsorbing anions and cations.
Acid-Base Disorders • Lungs can compensate immediately but: • the response is short term • and often incomplete. • The kidneys compensate are slower to respond (2-4 days) but: • the response is long term • and potentially complete
Metabolic (non-respiratory) Acidosis • Decrease pH, increase H+ • Bicarbonate decreased (<24 mmol/L) • Caused by: • acid producing substance or process • or reduce excretion of acids • Compensation: • 1o - Respiratory compensation: • Hyperventilation, decrease CO2 in circulation. • 2o -Renal compensation: • increase H ion loss by increasing H2PO4 and NH4 excretion and retain HCO3-
Respiratory Acidosis • Caused by hypoventilation • decrease the elimination of CO2 in the lungs, it builds up in the blood • decrease in pH, increase in H and HCO3 • Diseases: emphysema, drugs , congestive heart failure, bronchopneumonia. • Compensation • Renal compensation • increase H+ excretion& increase reabsorption of HCO3-
Metabolic (non-respiratory ) alkalosis • HCO3- increased, H+ decreased, pH increased • Causes of nonrespiratory alkalosis: • excess administration of NaHCO3 • ingestion of HCO3– producing salts such as Na-lactate, citrate or acetate • excessive loss of acid through vomiting • Compensation • Respiratory compensation • Hypoventilation with CO2 retention • Renal compensation • excrete HCO3- and retain H+ ions.
Respiratory alkalosis • Decreased CO2, decreased H+,increased pH • Causes of respiratory alkalosis include: • hypoxemia; • chemical stimulation of the respiratory center by drugs, such as salicylates (stimulate the respiratory center to cause hyperventilation); • pulmonary fibrosis. • Compensation • Renal compensation • decrease renal excretion of H+ ions, HCO3- excreted.