Download
1 / 16
160 likes | 178 Views
Explore case studies of patients with type 1 diabetes, including insight on identifying LADA and treatment strategies. Learn how healthcare professionals can manage and support individuals with this condition effectively.

E N D
Working with patients in primary care with type 1 diabetes Antonella Gilmour, NP-PHC November 13, 2015
Statistics Thanks to K Love who assisted with data collection
Insulin Therapy Delivery System 18 using insulin pump (47.4%) Avg A1C 7.86% 20 using multiple insulin injections (52.6%) Avg A1C 9.73%
So how does this relate to my experiences working with patients who have type 1 diabetes?
LADA Latent Autoimmune Diabetes in Adults
“LADA Phenomenon” • Identified in the 1970’s • Researchers were trying to prove that type 1 DM was an autoimmune disease by looking for auto antibodies • Found auto antibodies in patients with type1 and 10% of pts with type 2 • 2008 study in Diabetes found genetically LADA has features of both type 1 and type 2
Autoantibodies • Glutamic Acid DecarboxylaseAutoantibodies (GADA or Anti-GAD) • Insulin Autoantibodies (IAA) • Insulinoma-Associated-2 Autoantibodies (IA-2A) • Islet Cell CytoplasmicAutoantibodies (ICA) • Zinc Transporter 8 (ZnT8Ab)
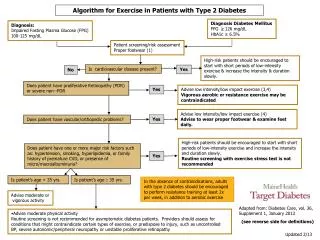
Why is it Important to Identify LADA? • Early insulin treatment may keep functioning beta cells • May provide insulin pump therapy as treatment option • Would allow SGLT2 for those that are not LADA
Case Study # 1 Ms. E.W. Generally healthy 35yr old female • G4T4 • BMI 24 • GDM requiring insulin (for last 10 weeks of her pregnancy which was 2 yrs ago) • father, brother, sister, paternal aunts x2, paternal uncle with type 2 DM • 2 months of ongoing vaginal yeast infections, blurry vision and 30 lb wt loss and feeling fatigue- still working FT • A1C 12.4%; no ketones in urine • No medications at present.
Outcome Visit 1- start metformin; discussed insulin as treatment option; urgent RD consult Blood sugars running mid 20’s 1 week later- phone f/u- blood sugars 12 ac meals and 17 pc meals Visit 2- 3 weeks later ; vision better; wt stable; ac meals 9-13; start basal insulin A1C 8.5% Visit 3- 1 month later- add apidra; insulin adjustments via phone calls A1C 6.0% (which was 6 mos after initial visit)
Case Study # 2 • Mr. R G • 26 yr old • Mental health- olanzapine x 5 yrs 12.5 mg • BMI 21; wt: 66.2kg; ht: 177.2cm • Polyuria, polydypsia, 20 lb unintentional wt loss • A1C 12.6%; office reading 29.4; no ketones in urine
Case Study # 3 • Mr. B J • Age 45 • Ht: 176 cm; wt. 70.6 • 20 lb unintentional wt loss over 3 mos; polyuria, polydypsia • Father type 2 DM • Smokes ½ ppd • A1c at 14.8% • Pancreatitis in past
Case study # 4 • Mr. T. S. • 51 yr old- diagnosed 12 yrs prior • Has been coming q3-4 mos for office visits • Started on basal insulin 5 yrs ago and rapid 3 yrs ago • A1c’s never below 7.6 • Wt; 84 kg; BMI 24; ht: 183