Download
1 / 37
370 likes | 496 Views
This presentation explores the critical dialogue between Course Directors (CD) and the Dean of Students regarding the early detection and management of student and resident challenges in medical education. Key objectives include understanding pre- and post-admission expectations, aligning academic standards, recognizing rights and responsibilities, and employing effective strategies to foster professionalism. With an emphasis on real-world scenarios, participants will learn to navigate common pitfalls in student behavior and ensure a supportive environment for academic success.

E N D
The Challenging Student and Resident Conversations between the CD and Dean of Students J. Mac Ernest, M.D. William P. Metheny, Ph.D.
Objectives • Discuss strategies for the early detection and documentation of student or resident problems • Recognize your rights and responsibilities as a CD or PD • Practice the application of strategies and responsibilities on actual scenarios
In the beginning… • What are the pre-admission expectations of your medical students? • What are the post-admission revelations of your medical students?
Pre-admission expectations • Knowledge • What should the student be able to learn (and how quickly)? • Skills • What technical standards does your school profess? • Attitudes • How do you expect the student to act, and what do you tell them about that?
Knowledge • Students (and CD) should be clear about academic expectations • Amount • Time within which to learn material • Repercussions of not learning material • Options when material is NOT learned
Skills • Does your school have technical standards clearly delineated? • Do you know them? • What are the physical requirements of your rotation that MUST be demonstrated in order to pass?
Attitudes • How does your school define/address professionalism? • Do you REALLY mean it? • Why should you care?
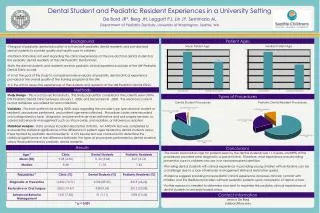
Simple administrative tasks and success • Students required to turn in a photo for pediatrics rotation • 29/366 (8%) who turned in photo, failed • 13/27 (48%) who did not, failed • Conclusion: • Organization and attitude are essential for success Wright, Tanner. BMJ 2002; 324: 1554-5
Does Medical Student Behavior Predict Professionalism Deficiencies in Practice? • “Failing to complete required course evaluations and failing to report immunization compliance were significant predictors of unprofessional behavior found by the review board in subsequent years.” Stern, Frohna, and Gruppen. Med Educ 2005;39:75-82
Does Medical Student Behavior Predict Professionalism Deficiencies in Practice? • “Problematic behavior in medical school is associated with subsequent disciplinary action by a state medical board.” Papadakis, Hodgson, Teherani, and Kohatsu. Acad Med 2004;79:244-249
Does Medical Student Behavior Predict Professionalism Deficiencies in Practice? • “Three domains of unprofessional behavior…were related significantly to later disciplinary outcome: • (1) poor reliability and responsibility; • (2) lack of self-improvement and adaptability; and • (3) poor initiative and motivation” Papadakis, Teherani, Banach, et al. NEJM 2005; 353, 25
Does Medical Student Behavior Predict Professionalism Deficiencies in Practice? • Poor reliability and responsibility • Unreliable attendance at clinic • Not following up on activities related to patient care • Diminished capacity for self-improvement • Unable to accept constructive criticism • Argumentativeness • Display of poor attitude • Poor initiative • Lack of enthusiasm or motivation • Passivity Papadakis, Teherani, Banach, et al. NEJM 2005; 353, 25
Post-admission revelations • What can a student be asked AFTER admission? • How should the information be used?
Americans with Disabilities ActADA; PL 101-336 • Signed by President Bush in July 1990 • Differs from Individuals with Disabilities Education Act-IDEA; 1975, PL 101-476 • Differs from Education for all Handicapped Children Act; 1975, PL 94-142 • Entitle children with disabilities to a free and appropriate education that allows for achievement • ADA evolved from Civil Rights Act of 1964 • Intended to eradicate discrimination in outcome-neutral environment
The ADA is a civil rights act, not an entitlement program • Student may qualify for accommodations in secondary school and not in college or medical school under the ADA • ADA should focus on equal opportunity and not on optimizing academic success • ADA guarantees that individuals who are otherwise qualified for educational programs or jobs will not be denied simply because they have a disability
How should a student with academic difficulties be evaluated? • Academic issues • Too much material, too difficult… • Processing • Learning disorder, ADD, don’t take tests well… • Distractions • Illness, family issues, personal issues, financial stress, abuse… • Motivation • Medicine was wrong career choice…
Requirements for effective system • Well-written bulletin • Clear technical standards • Stiff spined promotions committee • Dean who understands hierarchy of constituencies • Patients • School/Profession • Student
Prior To Clerkship • Do You Have any Prior Intelligence? • Regular CDs Meetings • Communication between coordinators • Comments from the dean of students • Notice from the student
Prior To Clerkship • Existing Policies Established by the CDs and Dean (e.g.,) • Absences from the clerkship • Professional code of conduct • Technical standards • Grading criteria and practices • Support from Dean for CDs
Orientation Make Explicit: • Goals, Objectives, Benchmarks • Grading Criteria and Evaluation Methods • Specific Assignments (see “Quiz”) • Work Ethic and Professional Conduct
Early Detection • Watch behavior at orientation! • Put mechanisms in place for faculty, residents, and students to contact you • Do a quick survey of the residents at the end of the 1st week • Call a student that the residents notice • Check at the end of the 1st week that students have started meeting reqs.
Midterm Assessment • LCME Requirement! • Conduct RIME meeting • Give Student Feedback and Forward • Have student repeat what to work on • Document mtg – what was discussed • Send a copy of note to student • Send a copy to Dean if warranted or expected • Put a copy of the note into student file
Problem Types* • Cannot Focus on What is Important • Has Poor Fund of Knowledge • Disorganized • Has Poor Integration Skills • Excessively Shy, Nonassertive • Overeager • Bright but Has Poor Interpersonal Skills • Uninterested • Too Casual and Informal • Avoids Work, No Show • Challenges Everything • “All Thumbs” • Con Artist, Rude, Hostile, Can’t Be Trusted • Psychiatric Problem • Substance Abuse Problem *J Med Ed 1987
What about Residents? • #1 Problem – getting documentation from residents and faculty of problems • Solutions: • Program Director should meet with the chief residents every week to discuss issues and resident adjustment • Chief residents must document problems (nothing 2nd hand) • Chiefs MUST handle with complete confidentiality • Chiefs MUST support the resident • PD should talk with Nurse managers at least once during a rotation where a resident is struggling • PD needs to sit down with the resident ASAP after data are collected. • Work out a step by step plan with the resident with deadlines. Have resident repeat back steps in the plan. Send notes and plan to resident. • Plan and resident should have a designated mentor to guide resident.
Scenarios • Academic • Technical Skills • Professionalism Questions: • What should happen at the clerkship level? • What should happen at the dean’s level? • What needs to be done for this resident?
ScenariosI. Academic Standards • Your grading system is composed of • Honors=“honors”: designated for top 15% of class • Pass=“satisfactory”: adequate performance • Low Pass=“less than satisfactory”: inadequate • Fail=“fail”: cannot progress without repetition • A fourth year student has received a grade of Low pass in every semester of each year and again receives a Low pass in your clerkship. This grade results in her being dismissed from school. She appeals, and states that, while her performance has not been stellar, she has technically “passed” all courses and rotations. She also has contacted one of your faculty members who has agreed to change his grade, which now results in a passing score in your rotation for this student.
ScenariosIIa. Technical Standards You get a call from an NP the 1st night of the clerkship that one of students has severe CP and is unable to glove or examine the patient. The Dean gave you no notice. Six weeks later she has not improved and is unable to perform the BPE on a SP. The Dean asks you to pass her if she just talks her way through the exam….
ScenariosIIb. Technical Standards MSIII says prior to clerkship he cannot perform pelvic exams because it is against his religious beliefs and in his culture only women are allowed to do them. He is willing to observe, just not examine. He is willing to do cervical checks however. He recruits the dean’s support to be excluded from this clerkship requirement.
ScenariosIIc. Technical Standards At the CDs mtg they discuss a student who is in her 7th year. She comes to your clerkship. The 2nd day residents complain she took nearly 5 hrs to write a H&P in triage. She states she is careful and that her eyes tire easily. She would like to be given more time than the other students to do her work. She appeals to the dean for his support.
ScenariosIIIa. – Professional Conduct A nurse contacts you that a MS-III is using the L&D computer to access a porn site. When questioned he states that it is actually a dating site showing scantily clad women. This student later presents his mother as his case presentation and admits he did the breast exam on her under resident supervision.
ScenariosIIIb. – Professional Conduct A MS-III wears a dreadlock tam on your clerkship. Most of the patients in clinic refuse to see him. You ask him to consider leaving it at home after you learn there is no religious basis – he just likes the look. He stops for 2 days then returns wearing it. In the clinic he later sits on the counter and kicks his feet in the exam room while the NP is counseling the patient….
ScenariosIIIc. – Professional Conduct • You learn that while on your rotation, a student got into an altercation with a police office who was investigating a fatal shooting of another police officer. The student was not involved in the shooting. When confronted, the student states that her activities off campus should be of no concern of yours, and does not understand why you as the CD would consider reporting the incident to the Dean of Students.
Resident Scenario I • Shortly after a resident starts the program the CNMs note that this resident spends an inordinate amount of time with each patient, talking about mostly social issues. This resident loves to teach medical students, always willing to drop what he is doing to teach. It also takes him extra time to write and dictate to the chart. He routinely exceeds the 80 hr work limit. He says the CNMs just do not like him.
Resident Scenario II • On her 1st ob rotation the new PG1 performs at her expected level except she is unreliable in her cervical exams. The CNMs give her every opportunity to practice including with simulations. Despite all efforts she shows no consistent improvements. She’s aware she is being scrutinized and gets worse in other areas. She comes to you to question if she is cut out for Ob/Gyn. What to do?