Download

1 / 68

E N D
Elevatedserum creatinine or proteinuria Before pregnancy CKD patients: whomshouldwefolllowin pregnancy? During pregnancy: Focus on the differentialdiagnosisbetween CKD and PE After pregnancy: Veryfew notes on the renalbiopsy
A 30 year old woman with kidney scars from previous acute pyelonephritis in the absence of GFR reduction, and on the contrary with a physiological hyperfiltration, no hypertension and proteinuria … Does it matter in pregnancy? Would we follow her? And how?
A 38 year old woman with SLE In remission on 10 mg/day prednisone, 100 mg Azathioprine, Well controlled hypertension (two drugs, ACEiand Ca antagonist) Proteinuria 1.3 g/day sCr 3 mg/dL; GFR 27 mL/min… Wait listed for pre-emptive kidney graft
How do we measure GFR define pregnancy related proteinuria and hypertension, on a background of CKD? How do the major determinants CKD (GFR, proteinuria and hypertension) play a role in pregnancy related morbidity? Do they share a hierarchic relationship? Whom should we follow, and how? When should we terminate a pregnancy or induce delivery? Is it there a risk threshold for “accepting” a pregnancy in CKD? How should we manage medically assisted procreation in CKD patients? Is a successful outcome an apparently healthy baby, in the arms of a mother who doesn’t need dialysis or renal transplantation in a next future? Are all CKDs alikein pregnancy?
Are all CKDs alikein pregnancy? Stages 1-2: 3% of women in childbearing age … 1:150-1:750 pregnancy is in stages 3-5… CKD: 20% in early PE…
Are all CKDs alikein pregnancy? The prognosis of pregnancy in CKD is not the same as in the general or “low-risk” population
Are all CKDs alikein pregnancy? The prognosis of pregnancy in CKD is not the same as in the general or “low-risk” population
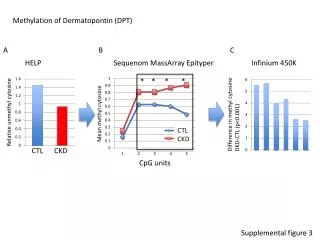
Table 2: Definitions and categories of the diseases What is the normal GFR? J Pregnancy. 2012; 2012: 105918.
Table 2: Definitions and categories of the diseases How do we measure Proteinuria? The existing evidence is not, however, sufficient to determine how protein to creatinine ratio should be used in clinical practice, owing to the heterogeneity in test accuracy and prevalence across studies. Insufficient evidence is available on the use of albumin to creatinine ratio in this area. Insufficient evidence exists for either test to predict adverse pregnancy outcome.
Beforepregnancy Beforepregnancy
A 30 year old woman with kidney scars from previous acute pyelonephritis in the absence of GFR reduction, and on the contrary with a physiological hyperfiltration, no hypertension and proteinuria … Does it matter in pregnancy? Would we follow her? And how?
what is the baseline risk? The general population? A “low risk” population? the risk for PE, a prototype of pregnancy related complications, is higher after kidney donation than before; Kidney donors are healthy…
Pre-term delivery: low-risk 4.9%; stage 1: 32.9%; stage 2: 40%; stage 3: 81.8%; stage 4-5: 100% Early pre-term: : low-risk 1.5%; stage 1: 14.8%; stage 2: 13.3%; stage 3: 54.5%; stage 4-5: 50% Need for NICU: low-risk 1.1%; stage 1: 18%; stage 2: 20%; stage 3: 54.5%; stage 4-5: 100%
Pre-term delivery: low-risk 4.9%; Stage 1: known diagnoses: 26.4%; new diagnoses: 30.9% Early pre-term: : low-risk 1.5%; stage 1 known diagnoses: 9.7%; new diagnoses: 10.9% Need for NICU: low-risk 1.1%; stage 1 known diagnoses: 14.1%; new diagnoses 14.6%
Is it possible to identify the “low-risk” CKD patients? The hyperfiltration hypothesis Analysis of our “best patients”: CKD stage 1; referredearly; non obese; non diabetic; non nephrotic; normotensive Stratificationaccording to GFR (EPI) at 10-14 weeks
Isitpossible to identify the “low-risk” CKD patients? The hyperfiltrationhypothesis No difference according to GFR; Significant differences versus low-risk controls: Preterm delivery 17.3% vs 4.9% need for NICU: 12% vs 1.1%
Is it possible to identify the “low-risk” CKD patients? The hyperfiltration hypothesis Working conclusion: take care of all stage 1 CKD patients. The effect of CKD is “qualitative” and not “quantitative”, merely linked to the intact parenchyma or to the intact capacity of increasing GFR… There is something missing…
How to take care of ourpatient? • Looking for the obvious… • Hypertension (teaching the patients to monitor blood pressure); • Proteinuria, detected from urinalysis; • Urinary tract infections, detected by urinary cultures and urinalysis • But how often?
How to take care of ourpatient? • In summary: • teaching how to control urinalysis and blood pressure; • Controlling urinary cultures every week, treating all of them, regardless of symptoms • “prophylaxis” with long term antibiotic therapy (Nitrafurantoin) in case of “several” positive urinary cultures. Blood and urinary tests, including kidney function every 1-3 months. • Kidney ultrasounds every 3 months • … Too much? • (similar frequency of controls in all stage 1 cases)
A 38 year old woman with SLE In remission on 10 mg/day prednisone, 100 mg Azathioprine, Well controlled hypertension (two drugs, ACEiand Ca antagonist) Proteinuria 1.3 g/day sCr 3 mg/dL; GFR 27 mL/min… Wait listed for pre-emptive kidney graft
How to take care of ourpatient? Start form the obvious Treat hypertension, without overtreatment (and discontinue ACEi and dangerous drugs…) Add aspirin (when??) Control urinary cultures, proteinuria GFR and urinary sediment (haematuria) Controlfoetalgrowth (2-4 weeks in “high risk” cases) Attention to weight gain…
How to take care of ourpatient? What else? In the absence of SLE relapse, In the presence of “normal” placentation, If blood pressure control is attained Weight gain is “regular” What about the “hyperfiltration” stress on the remnant nephrons (disease progression and proteinuria)? What about a “nephroprotective” diet?
How to take care of ourpatient? Can a low protein diet be a “substitute” for ACE inhibitors and ARBS in pregnancy?
How to take care of ourpatient? In the absence of reports on Alfa-kappa in pregnancy, efforts were made to control for risks linked to aminoacids, ketoacids and additives. No report had been found or made available by the company (Fresenius Kabi). Conversely, indirect evidence on “vegan pregnancy” and on supplements is searched… no harm if vitamins (B12, vit D) and iron are controlled and protein intake is at least 0.7-0.8 g/Kg/day
How to take care of ourpatient? Lowproteindiets: a crazy idea? Low protein diet employed in pregnancy consisted in an adaptation of the low-protein vegan diet employed in our centre. Our basic diet for non pregnant patients is vegan, with a protein intake of 0.6 g/Kg/day (ideal weight), 1-3 free meals per week, supplementation of 1 pill/8 Kg of ideal body weight. Caloric intake 30-35 Kcal/day. In an empirical attempt to balance the advantages of low-protein diets in CKD and the habit of increasing protein intake in pregnancy, we progressively adjusted the diet to 0.8 g/Kg/day of proteins, based on pre-conception weight, plus ketoacids (1:8 Kg). We progressively integrated the allowance of small quantities of milk and yogurt (100-150 mL), and changed the name to “vegan-vegetarian”, and the supplementation with vitamins B12, folate, vitamin D and iron, according to blood levels.
How to take care of ourpatient? 24 CKD patients with “severe proteinuria” or advanced CKD Indications: CKD stage 3b, or 3 a with diabetes or kidney transplant “severe proteinuria”: above 1 g/day in first trimester; rapidly increasing; nephrotic at any time 16 stage 3 “control pregancies” (milder disease, eating dsorders, late referral)
How to take care of ourpatient? Primum non nocere: First: do no harm Control for maternal outcomes
How to take care of ourpatient? Primum non nocere: First: do no harm Control for foetal growth Small for gestational age: 14% cases, 44% controls P=0.046
How to take care of ourpatient? • In summary: the obvious: • teaching how to monitor blood pressure; • Early aspirin; • Care to avoid rapid weight gain; glycaemia control • Controlling GFR, Urea, electrolytes, proteinuria, urinalysis, urinary cultures, blood cell count at least every other week. Immunologic testing every month. • And… • The less obvious: • Try a “moderate” vegan supplemented low protein diet
During pregnancy During pregnancy
A 34 year old woman, with no known history of renal disease, no known hypertension, is hospitalized at 25 gestational weeks because of symptomatic hypertension. At referral, serum creatinine is 3 mg/dL, proteinuria 4 g/day. Heamoglobin is 9 g/dL. The kidneys are normal-small (9 and 9.5 cm). The child is small for gestational age A previous urinalysis (20 weeks) displayed proteinuria ++ At that time BP was reported as 140/90; The data were overlooked until hospitalization CKD or PE: an emerging problem During pregnancy
PE: proteinuria >300 mg/day and hypertension developing after the 20th gestational week in a previously normotensive, non proteinuric woman. Normalization within 1-3 months after delivery. Is this preeclampsia? The patient did not know being hypertensive; hypertension was symptomatic Is this a (glomerular) nephropathy? The kidneys are normal-small; the data at 20 weeks doesn’t help. Is this “superimposed” PE? May be, but does the definition help? CKD or PE: an emerging problem During pregnancy
A 30 year old woman, diabetic since the age of 10 years; Laser treated retinopathy. Long follow-up in psychotherapy. Pregnancy termination at age 17. She started pregnancy with very good diabetes control (Hb1ac 6.5%), no proteinuria (0.12 g/day), normotension, GFR 110 mL/min, sCr 0.8 mg/dL This is a twin pregnancy (bicorial) She is well up to the 22nd gestational week when proteinuria suddenly rises to 1 g/24 hours and, within one week to 3.5 g/24 hours and to 11 g/day at the 26th week. GFR is normal; BP rises since 26th week. The male twin is affected by transposition of the great vessels. CKD or PE: an emerging problem During pregnancy
Growth of the children. Maternal creatinine and proteinuria CKD or PE: the emerging problem hypertension proteinuria creatinine
Is this preeclampsia? The patient is normotensive; the twins are developing normally… She developed mild hypertension two weeks later… Is this a diabetic nephropathy? The onset is abrupt. Diabetes control was “perfect” throughout pregnancy Is this “pregnancy induced proteinuria”? Indeed, but does the definition help? Is this another primary glomerulonephritis? May be, but these are twins CKD or PE: an emerging problem
What about… Pregnancy termination Selective termination of the pregnancy of the affected twin Kidney biopsy … What about… Albumin infusion Steroid treatment “Low” protein, low sodium diet Bed rest – hospitalization What is going on? CKD or PE: the emerging problem
In pregnancy: because the treatment may be different in PE and CKD; prognosis is usually better for CKD than for PE; PE: 2.4% of AKI 0.1% maternal mortality Why it is important to distinguish between PE and CKD?
Why it is important to distinguish between PE and CKD? After pregnancy: because a precise diagnosis of CKD is needed, and follow-up if any, is different
How to differentiate between PE and CKD? Pathologic uterine flows vs Normal uterine flows