Download
1 / 79
800 likes | 978 Views
Approach to Injuries of the Head & Spine. Stephan Brenner, MD, MPH. Teaching Objectives. By the end of this session you will learn: How to use the Glasgow Coma Scale (GCS). How to immobilize patients with the “Log-roll†maneuver . When to transfer patients with head or spine injuries.

E N D
Approach to Injuries of the Head & Spine Stephan Brenner, MD, MPH
Teaching Objectives By the end of this session you will learn: • How to use the Glasgow Coma Scale (GCS). • How to immobilize patients with the “Log-roll” maneuver. • When totransferpatients with head or spine injuries. • How to preparea patient with a head or spine injury fortransport.
Traumatic Head & Spine Injuries • Anatomy and of the brain and spine. • Mechanisms of head and spine injuries. • Assessment of head and spine injuries. • Treatment of the head or spine injured patient. • Referral or Discharge of head and spine injured patients.
Anatomy & Mechanism Case: • A young man is riding his motorbike when he hits a bump in the road. He is thrown off the bike. • He was not wearing a helmet and hit his head against a rock at the roadside. He is • unconscious for about 2 minutes. • He then is able to get up on his own and stops a passing car. The driver brings him to your casualty ward. How are we going to evaluate and treat this patient?
Anatomy & Mechanism: The Skull and Brain • The brain is surrounded by bones (skull). • The brain is connected to the spinal cord through a hole in the base of the skull.
Anatomy & Mechanism The Skull and Brain • Trauma can cause: • Intracranial bleeding orswellingof the brain. • Increased pressure inside the skull. • RisingIntra-Cranial Pressure (ICP) causes: • Squeezing of brain (=Herniation). • Altered mental status or coma. • Neurologic deficits
Anatomy & Mechanism Head Injuries • Causes: RTAs,falls, assaults. • Head injuries involving the brain are called Traumatic Brain Injuries (TBI). • TBI is a common cause of death in trauma patients! • TBI is a major cause of lifelong disabilityafter trauma!
Anatomy & MechanismTraumatic Brain Injuries (TBI) Immediate (= direct) brain damage: Once direct brain injury occurs, only symptomatic relief can be provided in the Casualty Ward (stabilization, prevention of further injury).
Anatomy & MechanismTraumatic Brain Injuries (TBI) Delayed (= indirect) brain damage: • Preventable brain damage in Casualty Ward after trauma occurs.
Anatomy & MechanismHead Trauma in the Casualty Ward THEREFORE: • Everyone working in the Casualty Ward needs to be familiar with the accurate assessment, resuscitation, and timely referral and transfer of patients with severe head injuries! • The survival and quality of life of every patient with head injury depends on the knowledge and skills of the Casualty Staff!
Anatomy & MechanismThe Spinal column Spinal column: • reaches from the upper neckto the lower back. • consists of 24 vertebral bones. • is divided into 4 sections.
Anatomy & MechanismThe Spinal column Spine Functions: Stability & Weight bearing Bone Structures • Vertebral bodies • Facet joints • Pedicles
Anatomy & MechanismThe Spinal column Spine Functions: Stability & Flexibility Non-bony Structures • Intervertebral Discs • Longitudinal Ligaments • Paraspinal Muscles
Anatomy & MechanismThe Spinal column • Spine Functions: Central Nervous System Nerve Structures • Spinal Cord • Nerve Roots • Spinal Nerves
Anatomy & MechanismThe Spinal Cord • Protected inside the Spinal Canal. • Originates from brain at the Foramen Magnum. • Terminates at Vertebra L1. • Distal nerve roots form the Cauda Equina inside the spinal canal below Vertebra L1.
Anatomy & MechanismThe Spinal Cord The 3 Major Spinal Tracts: • Corticospinal Tract motor control, muscle contraction. • Spinothalamic Tract pain and temperature sensation. • Posterior column position sense, vibration, light touch.
Anatomy & MechanismSpine Injuries Cervical Spine: • Most vulnerable part of spine • Involved in 50% of all spinal injuries! • High risk of paralysis from cord compression!
Anatomy & MechanismSpine Injuries Thoracic Spine: • Least vulnerable to injury (15% of all spinal injuries) • Relative protection from rib cage. Lumbar Spine: • 30% of all spinal injuries • Most injuries occur in the upper part of the L-spine (thoracolumbar junction)
Anatomy & MechanismSpine Injuries Causes: • High-velocity RTAs • Falls from a height • Sports injuries • Occupational injuries Mechanisms: • Whip-Lash Injury • (Flexion-Extension Injury) • Axial Compression Injury
Anatomy & MechanismSpine Injuries • Clinical Signs: You will never know what type of spine injury you are dealing with when a patient arrives to the Casualty Ward!!
Anatomy & MechanismSpine Trauma in the Casualty Ward THEREFORE: Nevertransport a patient with suspected spine injury in the sittingorprone position!! • Everybody working in the Casualty Ward needs to be familiar with how to assess and treat a patient with suspected spine injury! • The survival and quality of life of every patient with spine injury depends on the knowledge and skills of the Casualty Staff!
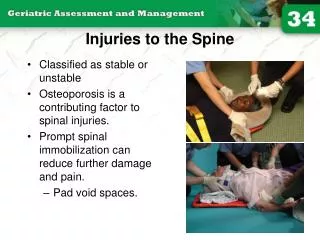
Anatomy & MechanismSpine Injuries Strains & Sprains: • Trauma to spine muscles and ligaments only. • Pain due to local soft tissue inflammation. Stable Spine Fractures: • Trauma to bone structures. • Only one column involved. • LOW RISK of spinal cord compression.
Anatomy & MechanismSpine Injuries Unstable Spine Fractures: • Trauma to bone structures. • More than one column involved. • HIGH RISK of spinal cord compression!
Anatomy & MechanismSpine Injuries Stable Fracture 1 column involved= low risk of spinal cord compression Examples of Stable Spine Fractures Wedge Fracture Transverse Process Fracture
Anatomy & MechanismSpine Injuries Unstable Fracturemore than 1 column involved = high risk of spinal cord compression Examples of Unstable Spine Fractures: Compression Fracture Flexion-Distraction Fracture
Anatomy & MechanismSpine Injuries REMEMBER! • In EVERY trauma patient, ALWAYS suspect an unstable spine fracture! THEREFORE: • ALWAYSprotect a trauma patient’s spine from bending or moving (= spine precautions)! BECAUSE: • Spinal cord damage is IRREVERSIBLE!!
Assessment & Treatment Case: • The motorbike accident patient arrives at the hospital and is walked to the Casualty Ward. • He complains about a headache and painin his neckandback. • He has bruises and abrasions to his face and forehead, shoulders and arms. Does he have a muscle sprain, or a stable spine fracture, or an unstable spine fracture? What next are the next steps in assessing him?
Assessment & TreatmentArrival to the Casualty Ward In any traumatically injured patient, the Casualty staff has to make sure that SPINE PRECAUTIONS are applied during every single step of the assessment & treatment process!
Assessment & TreatmentSpine Precautions Wrong methods!! Correct methods!!
Assessment & TreatmentSpine Precautions How to correctly apply Spine Precautions? • Place the patient in an anatomical position: • supine on a hard surface • straighten arms and legs • always support the head!
Assessment & TreatmentSpine Precautions • Immobilize the C-spine: • Achieve normal alignment of the cervical spine. • Instruct the patient not to bend or turn the head. • One person must support the patient’s head and neck until a cervical collar or other device is placed.
Assessment & TreatmentSpine Precautions Devices used to stabilize the C-spine: Sandbags (with a rolled towel beneath neck) Stiff Cervical Collar Rolled Towel
Assessment & TreatmentSpine Precautions • “Log-roll” the patient: • Turn the patient “in one piece” without moving the spine. • Requires at least 2 health care providers. • Must be used every time the injured patient has to be moved for examination or transport.
Assessment & TreatmentSpine Precautions “Log-roll” maneuver: • 1 provider stabilizes the headandneck. • All other providers turn the patient’s shoulders, hips, and legs.
Assessment & TreatmentPrimary Trauma Survey While applying Spinal Precautions,the Primary Trauma Survey exam is started. • A - Airway: Is the patient able to talk? • B - Breathing:Is the patient able to breath normally? • C - Circulation: Are the BP and PULSE normal? • D - Disability: Is the patient able to move all limbs? • E - Exposure: Are there any other visible injuries once the patient is undressed?
Assessment & TreatmentPrimary Trauma Survey • AIRWAY & BREATHING: Act accordingly! • Obstruction Clear Airway! • Labored breathing Position Patient! (while protecting C-spine) Intubate! (if appropriate) • Decreased one-sided breath sounds Needle Decompression! • Wheezing, Cyanosis Give Oxygen! Look for: • Foreign body in airway • Labored breathing • Blue skin (central cyanosis) Check for: • Airway obstruction • Decreased breath sounds • Wheezing
Assessment & TreatmentPrimary Trauma Survey CIRCULATION: Look for: • Cold Skin • Weak or Fast Pulse • Capillary Refill > 2 seconds Check for: • Low Blood Pressure • Fast Heart Rate • Active Bleeding • Act accordingly! • Cold skin • Keep patient warm! • Low BP, fast pulse Give 1 L NS or LR IV bolus! Repeat fluid bolus as needed! • Profuse Bleeding Pressure dressing to wound!
Assessment & TreatmentPrimary Trauma Survey • DISABILITY & MENTAL STATUS: Look for: • Unconsciousness • Head Injury • Patient moving all 4 limbs Check for: • AVPU or GCS score • Possibility of intoxication, • alcohol or drug abuse • Act accordingly! • Patient is unconscious Manage Airway! Intubate if appropriate! Check blood glucose level! • Seizure or Convulsion Give Diazepam IV or PR! • Low AVPU or GCS score, inability to move limbs • Spinal Precautions at all times!
Assessment & TreatmentPrimary Trauma Survey AVPU Score: Assessment of consciousness in non-trauma patients focus on a patient’s general responsiveness to certain stimuli. • A = patient is Alert & Awake • V = patient responds only to Verbal Stimulation • P = patient responds only to Painful Stimulation • U = patient is Unresponsive to any stimulation
Assessment & TreatmentPrimary Trauma Survey AVPU Example: A small boy fell off a tree and hit his head. In the Casualty Ward, he has his eyes closed and looks as if he is asleep. He does not respond when his mother calls his name. When the nurse pinches his hand, he screams and pulls his hand away. What is the boy’s level of consciousness according to the AVPU score?
Assessment & TreatmentPrimary Trauma Survey GCS = Glasgow Coma Scale: Assessment of consciousness in trauma patients assesses the patient’s specific responsiveness to certain stimuli in 3 elements of patient behavior. • Eye movements 4 points • Verbal response 5 points • Motor function 6 points A fully conscious patient has a GCS score of 15 points. Severe head injury is present with a GCS of 8 or below.
Assessment & TreatmentPrimary Trauma Survey Glasgow Coma Scale:
Assessment & TreatmentPrimary Trauma Survey GCS Example 1: A woman was seriously injured in a RTA and sustained severe head trauma. She does not open her eyes when rubbed on the chest, but she starts moaning, flexes both arms, and stretches her legs. What is this woman’s GCS score?
Assessment & TreatmentPrimary Trauma Survey GCS Example 2: A man involved in the same accident has been unconscious since the event. He does not open his eyes when rubbed on the chest, does not make any noises, turns both arms legs inward, and bends his hands and feet. What is this man’s GCS score?
Assessment & TreatmentPrimary Trauma Survey EXPOSURE (undress the patient!): Look for: • Additional wounds & injuries Check for: • Hypothermia • Act accordingly! • Wounds and Injuries cover open wounds! immobilize broken limbs! • Hypothermia cover the patient!
Assessment & TreatmentPrimary Trauma Survey Inform the physician or medical assistant on call immediately if any of the ABCDEs are abnormal!!
Assessment & TreatmentSecondary Trauma Survey 1) Obtain a detailed history from the patient or an eyewitness (AMPLE History): A= Allergies? M = Medications? P = Past Medical Problems? L= Time of Last Meal? E = Event – What happened? – What mechanism?
Assessment & TreatmentSecondary Trauma Survey • Do a detailed Physical Exam from head to toe, specifically looking for the following: • Dilated or unequal pupils. • Leakage of Cerebrospinal Fluid. • Detailed neurologic exam (sensation, motor function, reflexes). • Log-rollto check for trauma to back of head, spine tenderness, bruising, step-offs.
Assessment & TreatmentSecondary Trauma Survey Signs of C-spine Injury: • Difficulties breathing damage to phrenic nerve • Flaccid upper extremities& loss of reflexes damage to anterior spinal cord • Hypotension & bradycardia damage of the autonomic nervous system
Assessment & TreatmentSecondary Trauma Survey • Decreased abdominal wall tone damage at level of T-spine • Decreased sensation or motor function in lower limbs damage at level of L-spine • Decreased rectal tone damage at level of L-spine