Download
1 / 49
560 likes | 1.01k Views
The Role of PARP inhibitors in Breast Cancer. QROC November 5 th , 2010 Rebecca Dent, MD FRCP(C) Sunnybrook Odette Cancer Center Toronto, Canada. Potential Conflict of Interest. Dr. Rebecca Dent AstraZeneca, consultant and honorariat (2007-2010)

E N D
The Role of PARP inhibitorsin Breast Cancer QROC November 5th, 2010 Rebecca Dent, MD FRCP(C) Sunnybrook Odette Cancer Center Toronto, Canada
Potential Conflict of Interest • Dr. Rebecca Dent • AstraZeneca, consultant and honorariat (2007-2010) • Roche, consultant and honorariat (2007-2010) • Sanofis-Aventis, consultant and honorariat (2007-2010)
Why did the Scientific Committee ask the young investigator from Sunnybrook to talk about PARP inhibitors in breast cancer? Two Reasons: Smallest study evaluating PARP inhibitors (but provocative!) Large clinical practice of TNBC and BRCA mutation carriers
Achilles’ Heel: A deadly weakness in spite of overall strength, that can actually lead to downfall
Neoadjuvant endocrine responses in ER + disease can be prolonged and gratifying at very little cost! Can we do this for triple negative and BRCA related cancers?
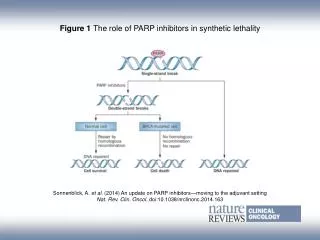
PARP inhibitors – Finding the Achilles’ Heel in BRCA related Cancers
BRCA2+/+ BRCA1+/+ BRCA2+/- BRCA1+/- BRCA1-/- BRCA2-/- Increased sensitivity of BRCA1-/- and BRCA2-/-cells to PARP inhibition No difference in sensitivity between heterozygous and wild-type BRCA cells Targeted inhibition selective and less toxic therapy Farmer et al. Nature 2005; 434:917-21
OlaparibA novel, orally active PARP inhibitor A phase I trial identified olaparib (AZD2281; KU-0059436) 400 mg bid as the maximum tolerated dose1 with a signal of efficacy in BRCA-mutated ovarian cancer • Most common toxicities: CTCAE grade 1 and 2 nausea and fatigue • Significant PARP inhibition and tumor response at olaparib doses 100–400 mg bid 1. Yap T et al. J Clin Oncol 2007;25(18S):abst 3529; 2. Fong P et al. J Clin Oncol 2008;26(15S):abst 5510.
Phase II trial of Olaparib in BRCA-deficient advanced breast cancer To assess the efficacy and tolerability of oral olaparib in BRCA1/ BRCA2 mutation carriers with breast cancer Multicenter proof-of-concept phase II study, single-arm sequential cohort design *Following an interim review of the emerging efficacy of each cohort, patients ongoing in 100mgbid cohort were permitted to crossover to receive the 400 mg bid dose Confirmed BRCA1 or BRCA2 mutation Advanced refractory breast cancer(stage IIIB/IIIC/IV) after failure of ≥1 prior chemotherapy for advanced disease Cohort 1 (enrolled first) Cohort 2 * Olaparib 400 mg po bid (MTD) 28-day cycles; n=27 Olaparib 100 mg po bid 28-day cycles; n=27 Tutt A. et al. Lancet 2010
Efficacy Olaparib 400 mg bid (n=27) Olaparib 100 mg bid (n=27) ITT cohort 6 (22)* 0 6 (22) Overall Response Rate, n (%) Complete Response, n (%) Partial Response, n (%) 11 (41)* 1 (4) 10 (37) *An additional 1 patient in the 400 mg cohort and 3 patients in the 100 mg cohort had unconfirmed responses Tutt A. et al. Lancet 2010
Olaparib 100 mg: 3.8 (1.9–5.5) months NB: Non-randomized sequential cohorts 100 mg: 27 25 17 10 4 0 0 0 0 0 Progression-free survival 100 Median PFS (95% CI) 90 Olaparib 400 mg: 5.7 (4.6–7.4) months 80 70 60 Freedom from progression (%) 50 40 30 20 10 0 0 50 100 150 200 250 300 350 400 450 PFS (days) No. of patients at risk 400 mg: 27 26 22 17 13 8 6 5 1 0 Tutt A. et al. Lancet 2010
* * * * * * *Prior platinum Tx Best % change from baseline in target lesions by prior chemotherapy Olaparib 400 mg bid cohort 100 Previous anthracycline, taxane and capecitabine 80 60 Increasing tumor shrinkage 40 Best % change from baseline 20 0 –20 –40 –60 –80 –100 Tutt A. et al. ASCO 2009
Response by BRCA mutation status and hormonal statusCohort: Olaparib 400mg BID Tutt A. et al. Lancet 2010
Adverse events* Olaparib 100 mg bid (n=27) Olaparib 400 mg bid (n=27) Grade 1/2 Grade 3 Grade 3 Grade 1/2 Patients, n (%) 15 (56) 11 (41) 7 (26) 10 (37) 6 (22) 8 (30) 4 (15) 1 (4) 2 (7) 2 (7) Fatigue Nausea Vomiting Headache Constipation Diarrhea Cough Dyspnea Insomnia Pain in extremity 4 (15) 5 (19) 3 (11) 0 0 0 0 0 0 0 15 (56) 15 (56) 6 (22) 5 (19) 8 (30) 4 (15) 8 (30) 10 (37) 7 (26) 6 (22) 2 (7) 0 0 1 (4) 0 0 0 1 (4) 0 1 (4) *≥25% reported in either cohort; Common Terminology Criteria for Adverse Events
Olaparib Phase2 - Conclusions In BRCA mutation carriers: single agent oral olaparib 400 mg bid has substantial activity with ORR 41% and median PFS 5.7 months well tolerated Not all patients with BRCA mutations responded Are there different Homologous Recombination Repair Defects affecting sensitivity to PARP inhibition? Is there something else that predicts response to PARP inhibition? Likely need functional assay! Perhaps subtypes of sporadic breast cancer may benefit from PARP inhibitors
Phase II Study of oral Veliparib Plus Temozolomide in Metastatic Breast Cancer aORR + stable disease Efficacy appears to be restricted to BRCA1/2 mutation carriers. Further evaluation of this combination is ongoing in BRCA1/2-mutated cancers. Isakoff et al. J Clin Oncol 2010; 28(suppl):118s (abstract 1019).
Phase II Study Veliparib (ABT-888) + Temozolamide • ORR: 7% • All BRCA1/2+ (RR 38%) • Toxicity: • marrow, nausea, electrolyte, fatigue • no gr3-4 after dose change ABT888 * = BRCA carriers % change * * * * * * p-value = 0.0042 Carriers: Median PFS = 5.5 Mo Noncarriers: Median PFS = 1.8 Mo Isakoff et al, ASCO 2010
Proof of Concept Phase 2 trials • Studies with Olaparib and Veliparib confirm that BRCA related cancers deficient in specific aspects of DNA repair are sensitive to agents that exploit this pathway, unless resistance occurs... • Major mechanism of resistance ...not in PARP genes but ...re-expression of a functional form of BRCA2 and in some cases almost the full-length protein
Resistance to PARP inhibitorsReversion of BRCA2 mutations Restoration of the open reading frame of BRCA1 or 2 by intragenic deletion Partial function of BRCA is restored and cells become competent for HR repair Edwards et al. Nature 451: 1111-1115, 2008
Cisplatin Resistance in tumors • Ovarian tumors with BRCA2 mutations highly sensitive to cisplatin but resistance develops • Analysis of resistant tumor line revealed reversion of BRCA2 mutation as with PARP inhibitors Implications: -Phase 2 Olaparib study showed that pts who progressed on platinum therapy rarely responded to Olaparib =but too soon to conclude cross-resistance Sakai et al. Nature 451:1116-1120,2008
What is the Role of PARP inhibitors in Triple Negative Breast Cancer?BRCA and TNBC
Theorem: • Shared genome-wide expression array patterns between BRCA1-mutant and basal breast cancer may reflect shared defects in DNA repair processes • Corollary: • Sporadic basal breast cancers may be especially sensitive to DNA-damaging agents
TNBC Shares Clinical and Pathologic Features with BRCA-1-Related Breast Cancers *BRCA1 dysfunction due to germline mutations, promoter methylation, or overexpression of HMG or ID44 1Perou et al. Nature. 2000; 406:747-752 2Cleator et al.Lancet Oncol 2007;8:235-44 3Sorlie et al. Proc Natl Acad Sci U S A 2001;98:10869-74 4 Miyoshi et al. Int J Clin Oncol 2008;13:395-400 26
Platinum Sensitivity in BRCA1+/TNBC:Pathologic Response to Neoadjuvant Rx BRCA1+: • 102 BRCA1+ patients • CDDP 75 mg/m2 x 4 • BUT retrospective • CDDP cohort – smaller, more node-negative Byrski, JCO 2009 • Triple negative: • 28 TNBC • CDDP also 75 mg/m2 x 4 • Prospective trial • 2/2 BRCA1+ had pCR Silver, JCO 2010
Case LG • 51F, known BRCA1 mutation carrier • right sided LABC, TNBC • Treated with Epi/Taxotere x6 on clinical trial • Mastectomy December 2008, with residual 1cm of IDC, 2/19LN + • Feb 2010 • Matted ipsilateral supraclavicular, cervical nodes • Brachial plexopathy due to extensive deep axillary recurrence causing severe pain requiring extensive narcotics
LG continued • Treated as part of TRIO trial with Taxotere +/- IMCLONE antivegf molecule • Radiological Response at 6wk CT scan • However, by clinic visit pt had extensive skin progression and pain requiring Gabapentin 900mg TID and Hydromorphone Contin 12 TID • April 2010: Started on Cisplatin 25mg/m2, Gemcitabine 750mg/m2 IV 3 out of 4 weeks • After one cycle pt was off all hydromorphone and tapering gabapentin, has just completed cycle 8 with almost complete response!
Case CH • 49F previously well, BRCA negative • 2cm, grade 3, 8/19LN+ TNBC • Treated with dd AC-paclitaxel • Completed August 2009 • November2009 • Acutely unwell, fatigue, jaundice • Abdominal ultrasound confirms diffuse liver metastases with no evidence of obstruction • Started on Cisplatin 25mg/m2 IV 3 out of 4 weeks
Case CH Why did she respond and so quickly to single agent weekly cisplatin? Why did she unfortunately respond for only four months? Need biopsies!
Canadian Study 20Phase II Trial of Olaparib in BRCA and sporadic breast and ovarian CA • Goals • To determine markers of response and resistance to Olaparib in four cohorts of patients • To help inform future studies in terms of patient enrollment • To help determine activity Gelmon K et al ASCO 2010
Study Design: 2-stage Simon Screening/enrolment Known BRCA + ovarian cancer (n=10) Known BRCA + breast cancer (n=10) HGSC with unknown BRCA status (n=15) TNBC with unknown BRCA status (n=15) ³ 1 response ³ 1 response + 40 patients = (n=55) + 20 patients= (n=35) Olaparib 400 mg bid TNBC, Triple-negative breast cancer; HGSC, High grade serous ovarian carcinoma
Best % Change in Target Lesion Size by Tumor Type and BRCA status: Breast Cancer 120 100 TNBC BRCA TNBC non-BRCA 80 Non-TNBC BRCA 60 40 20 Best % change from baseline 0 –20 –40 –60 • 23 treated patients with target lesions identified at baseline • 22 had at least one follow-up assessment • 1 patient had no follow-up tumour size assessment • 1 due to missing / incomplete post-baseline assessments –80 –100 No patient met the criteria for a confirmed RECIST response Best change in target lesion size is maximum reduction from baseline or minimum increase in absence of reduction
Phase I safety cohort: Olaparib plus Paclitaxel for TNBC TN metastatic breast Ca ≤1 prior cytotoxic therapy Olaparib (AZD2281) 200 mg BID po + Paclitaxel weekly iv 90 mg/m2 (3 of 4 weeks) Safety cohort N=19 • Primary objective: • Safety and tolerability • Secondary objectives: • Objective response rate (ORR) according to RECIST Dent R et al. ASCO 2010
CTCAE in ≥30% of patients overall Patients with AEs, n (%) CTCAE, Common Terminology Criteria for Adverse Events
Phase I/II Study of Olaparib Plus Paclitaxel for Triple-Negative Metastatic Breast Cancer • Eligibility: ≤ 1 prior cytotoxic regimen • Regimen: olaparib 200 mg p.o., b.i.d. • paclitaxel 90 mg/m2/week 3 of 4 weeks Dose modifications: Median dose intensity (total dose received/total dose planned) of paclitaxel was 57.2% (range 26–100%) in cohort 1 and 73.1% (range 29–100%) in cohort 2 Conclusions: Olaparib/paclitaxel is active in triple-negative MBC. Associated neutropenia reduced paclitaxel dose intensity Dent et al. J Clin Oncol 2010; 28(suppl):118s
Lessons from Study 11 • Other than neutropenia, well tolerated therapy • Little to no neurotoxicity, is this related to other physiological roles of PARP? • Other Important Observations • Patients exhibited delayed response to Olaparib (implications for neoadjuvant studies with PARPi) • Differential response to treatment (response in lung, progression lymph nodes) – implications for clinical trials • Expansion cohort evaluation different schedules of Olaparib Dent, R et al . ASCO 2010
LBA11 Iniparib Study Design Multi-center, open-label, randomized Phase II • Metastatic TNBC -about 70% had prior chemotherapy for early BC • Measurable disease -median number of metastatic sites = 3 • 0-2 prior chemotherapy regimens for metastatic disease - no prior chemo~60% • No prior gemcitabine, carboplatin, cisplatin, PARP inhibitor • Stable brain metastases allowed • ECOG PS 0–1 - two thirds PS = 0 Randomization (1:1) Gemcitabine1000 mg/m2, IV, d 1, 8 CarboplatinAUC 2, IV, d 1, 8 21 day cycles Iniparib 5.6 mg/kg, IV, d 1, 4, 8, 11 Gemcitabine 1000 mg/m2, IV, d 1, 8 Carboplatin AUC 2, IV, d 1, 8 21 day cycles N=62* RESTAGING: Every 2 Cycles (RECIST) N=61 PRIMARY ENDPOINTS: CBR = CR + PR + SD ≥6mo, Safety SECONDARY ENDPOINTS: DFS, ORR, Toxicity *30 patients randomized to gem/carbo crossed over to receive gem/carbo + Iniparib (BSI-201) at disease progression
Iniparib: Response and Clinical Benefit Rates (ITT Population) *P-values were not adjusted for multiple interim analyses.
Iniparib: Progression-Free and Overall Survival (ITT Population) Progression Free Survival Overall Survival-Exploratory PFS + 2.3 months OS + 4.6 months *P-values were not adjusted for multiple interim analyses.
Summary • Proof of Concept that triple negative breast cancers may be susceptible to PARP inhibition • Impressive improvement in ORR, CBR , PFS and overall survival • BSI-201 + gemcitabine/carboplatin was well tolerated and did not potentiate chemotherapy-related toxicities
Questions • Are the platinum and PARP inhibitor effects additional or synergistic? What is the activity of single agent BSI-201 in pts with TNBC? • Why does BSI-201 not show significant myelosuppresion compared to oral PARP inhibitors?
Development in PARP inhibitors in TN Breast Cancer Challenges Triple Negative Breast Cancer Defining Triple Negative Breast Cancers Identifying Subset with Homologous Recombination Deficiency What are the Standards of Care for Treatment? What should be the comparators? PARP inhibitors Dosing: IV vs. PO Schedule: Intermittent vs. Continuous Timing: Delivery before, during or after chemotherapy Are they best combined with DNA damaging agent? Role of Resistance
Acknowledgements and Collaborators CANADA Maureen Trudeau Steven Narod Karen Gelmon Mark Clemons Wedad Hanna Janet Dancey Kathy Pritchard UK Andy Tutt Alan Ashworth AstraZeneca Lynn Douglas Mark Zarenda Ursula Lotz Jim Carmicahel
2011 Triple Negative Breast Cancer Conference, March 9-11, London UK Scientific programme committee • Alan Ashworth, Jorge Reis-Filho, Rebecca Dent and Andy Tutt Speakers • Charles Perou • Will Foulkes • Jos Jonkers • Gabriella Dontu • Matt Ellis Speakers cont.. • Judy Garber • Steven Narod • MikeStratton • Lajos Pusztai • Anne Vincent-Salomon, • Andrea Richardson • Max Parmar