Download
1 / 33
390 likes | 678 Views
ABRUPTIO PLACENTA. ANTEPARTUM HEMORRHAGE DEFINITION. Bleeding from or into the genital tract after the 28 th weeks of gestation but before the birth of the baby. - D C. Dutta. CAUSES OF ANTEPARTUM HAEMORRHAGE. PLACENTAL BLEEDING Placenta previa

E N D
ANTEPARTUM HEMORRHAGE DEFINITION Bleeding from or into the genital tract after the 28th weeks of gestation but before the birth of the baby. - D C. Dutta.
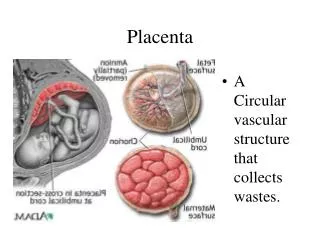
CAUSES OF ANTEPARTUM HAEMORRHAGE • PLACENTAL BLEEDING • Placenta previa • Abruptio placenta • UNEXPLAINED • EXTRA PLACENTAL CAUSES • Local cervico-vaginal lesions • Cervical polyp • Carcinoma cervix • Varicose vein • Local trauma
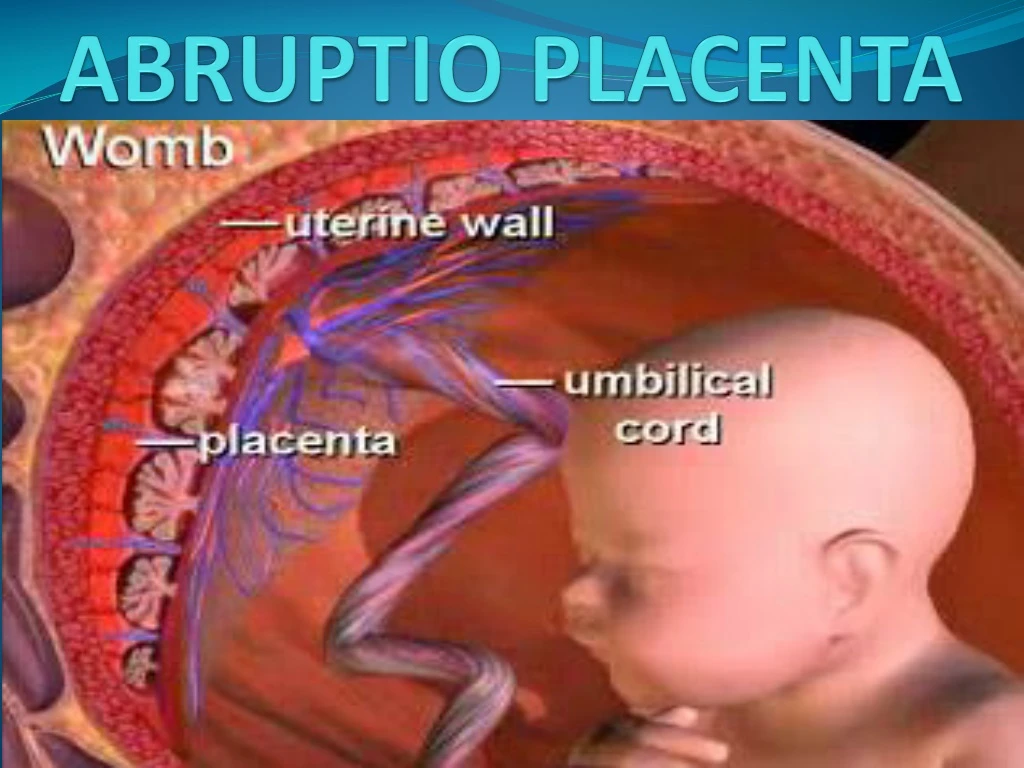
ABRUPTIO PLACENTAE A latin word “Abruptio placentae” means “Rending asunder of placenta”, which means ‘a sudden accident’
DEFINITION Bleeding occurs due to premature separation of normally situated placenta after 28 weeks of gestation and before the birth of the baby. - Williams.
INCIDENCE • 1 in 150 deliveries which resulted death of fetus • 1 out of 500-750 deliveries lead to maternal mortality about 2-5%
ALTERNATIVE NAMES • Premature separation of placenta • Accidental haemorrhage • Ablatioplacentae • Abruptio placentae • Placental abruption
TYPES • REVEALED • CONCEALED • MIXED
ETIOLOGY PREVALANCE IS MORE WITH • High birth order • Advancing age of mother • Poor socio-economic condition • Malnutrition • Smocking
ETIOLOGY.....Contd • Hypertension in pregnancy • Trauma • Sudden decompression • Short cord • Supine hypotensive syndrome • Placental anomaly
ETIOLOGY.....Contd • Sick placenta • Folic acid deficiency • Uterine factor • Torsion of the uterus • Cocaine abuse • Thrombophilias • Prior abruption
PATHOGENESIS • Due to etiology Hemorrhage into decidua basalis Decidua splits Development of decidual hematoma Separation, compression, ultimate destruction of placenta.
Contd… 2. Decidual spiral artery ruptures Retroplacental hematoma forms Expands with increase in bleeding. Area of separation rapidly becomes extensive & reach margins Uterus unable to contract & compress vessels Blood dissect membranes from uterine wall
CLINICAL CLASSIFICATION: • Grade 0 • Clinical features absent • Grade I • Bleeding slight • tender and irritable uterus • Maternal Bp and fibrinogen level unaffected • FHS good. • Grade II • Bleeding moderate • uterus tender • shock absent • fetal distress present. • Grade III • Bleeding severe • uterus tender • shock present • fetal death is ruled • coagulation defect or anuria.
MANAGEMENT PREVENTION: Aims - >Eliminate risk factors >Correct anemia >Prompt detection & treatment >Avoid trauma >Avoid sudden decompression of uterus >Avoid supine hypotension >Routine Folic acid administration
-Rush to well equipped maternity unit as early as possible……… Treatment: AT HOME:
I. REVEALED TYPE: • Assessment of case • Assess amount of blood loss • Assess maturity of fetus • Assess whether in labour or not • Presence of any complication
Preliminaries • Sent blood for Hb%, coagulation profile, ABO, Rh grouping. • Urine for protein. • Ringer’s solution drip & arrange for blood transfusion. • Close monitoring of mother & fetus *Use Large Bore IV Lines*
Definitive Treatment: • Patient in labour – Accelerate labour - Oxytocin drip. APH = ARM
Contd… • Patient not in labour – • Pregnancy 37 wks or more • Induction of labour by low ARM • Caesarean section - fetal distress - complications - control bleeding fails
B. Pregnancy less than 37 wks – • Bleeding moderate to severe & continuing -ARM - Oxytocin drip - C. S • Bleeding slight & has stopped - conservative treatment -close monitoring
II . MIXED or CONCEALED: Principles; • To correct hypovolemia & to restore blood loss • To bring effective uterine contraction & termination of abruption process • To observe blood coagulation profile • Close monitoring
Definitive Treatment: • Blood investigation • To correct hypovolemia • AROM with oxytocin • Vaginal delivery • Caesarean section
COMPLICATIONS: • HAEMORRHAGE • SHOCK • BLOOD COAGULATION DISORDERS • OLIGURIA & ANURIA • POSTPARTUM HAEMORRHAGE • PUERPERAL SEPSIS • ISCHAEMIC NECROSIS
COUVELAIRE UTERUS • Massive intravasation of blood into the uterine musculature upto the serous coat • Condition diagnosed on laparotomy • Uterus is of dark port wine color may be patchy or diffuse • Starts at cornu then spread to other area • Hemorrhage are found under the uterine peritoneum and may extend into the broad ligament • Myometrial hematoma interferes with uterine contractions
Fetal Risks • PERNATAL MORTALITY • GROWTH RESTRICTION • CONGENITAL MALFORMATION • ANAEMIA
Nursing Management: • Monitor vital signs & record • Assess amount of blood loss • Assess contraction pattern • Assess urine output &skin color • Send for cross matching & grouping • Administer Morphine if pain present • Put wide bore IV line or CV line • Physical comfort & emotional support • Check fundal height & abdominal girth • Monitor fetal well being