Download
1 / 27
270 likes | 628 Views
Oral anticoagulants and regional anesthesia for joint replacement surgery. Reported by R1 康庭瑞 2002/11/5. Case present . Identifying data Name: 王 X 傭 Age: 73 years old Gender: male Chart number: 2000625 Bed number: 11B11-1 Operative day: 2002.10.28. Brief history. Chief complaint:

E N D
Oral anticoagulants and regional anesthesia for joint replacement surgery Reported by R1 康庭瑞 2002/11/5
Case present • Identifying data • Name: 王X傭 • Age: 73 years old • Gender: male • Chart number: 2000625 • Bed number: 11B11-1 • Operative day: 2002.10.28
Brief history • Chief complaint: Right knee walking pain for more than 1 month • Present illness: • Falling down and right knee was injured years ago. • Intermittent right knee pain and soreness, poor weight bearing • Severe varus deformity and osteoarthritis with joint space narrowing
Brief history • Past history: • Heart disease with 3VD s/p CABG 2 years ago at 振興 hospital • Denied of DM, liver, renal, lung diseases • Drug and food allergy: denied • Previous operation history: (1) CABG 2 years ago. (2) Gall bladder stone s/p. (3) Cataract s/p • Smoking (+)– 1~2 PPD, alcohol comsumption– denied
Brief history • Current drugs: • Bokey (Aspirin): 100㎎ • Lipitor (Atorvastatin) • Mirobect (Atenolol) • Imdur (Isosorbride 5-mononitrate) • Lasix, spironolactone • Narcaricin (Benzbromarone)
Brief history • Physical examination • Consciousness: clear • Vital sign: T/P/R—36.5/60/15 BP—100/60㎜Hg • BW:55.2㎏, BH: 152㎝ • HEENT: conjunctiva—pink, JVE—nil • Chest: symmetric expansion, breathing sound—clear • Heart: NSR, no murmur • Extremities: no pitting edema
Laboratory data: (2002.10.27) Blood type: O, Rh(+) WBC: 6310 RBC: 344 Hb: 11.1 PLT:205 Bilirubin T: 0.31 GOT: 16 BUN: 42.5 Creatinine: 2.34 Na: 139 K: 4.89 Cl: 102 Sugar AC: 136 Brief history
Discussion • Regional anesthesia and anticoagulation–Journal of clinical anesthesia, February 2001 • Update on spinal anesthesia–Anesthesiology, May 2001 • Spinal-epidural hematoma following epidural anesthesia in the presence of antiplatelet and heparin therapy–Anesthesiology, October 2001
Discussion • Oral anticoagulants and regional anesthesia for joint–regional anesthesia and pain medicine, January-February 2002 • Epidural anesthesia prevents hyper-coagulation in patients undergoing major orthopedic surgery–regional anesthesia and pain medicine, May-June 2002
The use of regional anesthesia and analgesia in the presence of anticoagulation has always been a controversial issue • Incidence of spinal hematoma with spinal anesthesia without anticoagulation is estimated at 1:220,000small surveys, anecdotal reports, and expert opinion • Anticoagulants used in the surgical population as prophylaxis and treatment for thrombotic condition
Review of commonly used anticoagulants • Antiplatelet drugs– inhibit platelet function • Aspirin(ASA): irreversible inactivates COX, even low-dose aspirin (40~81㎎) may suppress TXA2 synthesis & PLT aggregation, inhibiting 1 hr after ingestion, entire lifespan≒10 days • Newer generations: inhibiting ADP-induced PLT aggregation (entire lifespan) or PLT GPIIb/IIIa receptor (48 hrs) • NSAIDs: reversibly and competitively inhibit COX, duration is dose-dependent and half-life of the NSAID
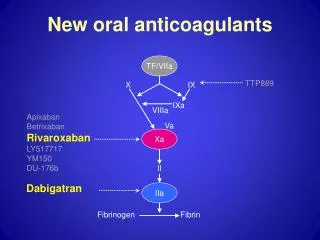
Review of commonly used anticoagulants • Oral anticoagulants (Warfarin) • Interfering with the Vit. K-dependent coagulation protein, factors II (thrombin), VII, IX, and X • Inhibiting Vit. K reductases, depletes Vit. KH2, and limits carboxylation • PT and INR may not accurately measure true antithrombotic activity • A decrease in factors II and X (longer half-life) is more important for the antithrombotic efficacy of warfarin
Review of commonly used anticoagulants • Heparin • Binding with antithrombin III, which accelerates inactivation of factors II, IX, X, XI and XI • Mixture of polysaccharide chains, MW ranging from 5,000 to 30,000; the length of the heparin chain determines which factor will be inhibited • Extensive binding to plasma proteins complicated the pharmacokineyics of heparin
Review of commonly used anticoagulants • LMWH has relatively greater anti-Xa activity, more predictable bioavailability and longer half-life • PTT doesn’t accurately reflect the degree of anticoagulation, factor X levels don’t correlated with potential for bleeding
Regional anesthesia and anticoagulants • Concurrent use of other anticoagulants increasing the risk of bleeding complication without influencing standard laboratory test • Minimize the degree of sensory and motor deficit of the analgesic regimen • Epidural catheters should be removed at the nadir of anticoagulant therapy • Routine continued neurologic monitoring for at least 24 hours
Regional anesthesia and antiplatelet medications • 1,000 patients undergoing orthopedic procedures while taking anti-PLT drugs and 1,800 obstetric patients with low-dose aspirin(60㎎) received neuraxial anesthetic and no hematoma were noted • Review of all reported cases of neuraxial hematoma from 1906 to 1994, only 4 of 61 cases were associated with the use of anti-PLT drugs, and 3 use of another anticoagulant
A case report • 63-yr-old woman(165㎝;75㎏), ASA class III, for reimplantation of a prosthesis of the right knee • One subcutaneous injection of LMWH (nadroparin,3800IU/day) as a prophylactic antithrombotic treatment (12hrs before surgery) • Pre-OP, PTT:33s(30~40s), PT:84% (70~120%), INR:1.01 (therapeutic level 2~4.5), PLT count:151*109/L (150~400)
Epidural puncture and insertion of the catheter were uneventful • Combined regional and general anesthesia was induced • At the end of surgery, continuous epidural infusion of 0.25% marcaine (8ml/h) was initiated. LMWH was reestablished 6h after the end of surgery • 18hrs later, epidural infusion rate↑to 12ml/h and 2 boluses of 12ml marcaine given for surgical and back pain • 400㎎ ibuprofen rectally for back pain • Painful during injection→remove catheter ≒7h after 2nd post-OP LMWH given
At that time, the coagulation parameters were within normal range, PLT count was 118*109/L • After removal, she received PCA • 10hrs after removal, back pain↑and voiding difficulty,↓muscle strength and sensation in both lower limbs • MRI revealed a spinal-epidural hematoma from T10 to L4 • Emergency decompressive surgery→ partially organized and fresh • No neoplastic changes or vascular malformations • Specific drugs taken per-OP:500㎎ QID ibuprofen on her own for arthritic pain and the last dose≒10h before surgery
High dose ibuprofen and a single dose • Lower limit of normal range PLT count, and decreased after surgery • 2 subcutaneous injection of LMWH before catheter removal • Back pain as an early symptom can be absent with continuous epidural analgesia. Insufficient analgesia was probably the first clinical sign • German society of anesthesiology and intensive care medicine: free interval of 1~2 days after NSAID, and at least 3 days without ASA-containing medication for central neuraxial manipulation
Epidural anesthesia prevents hyper-coagulation in patients undergoing major orthopedic surgery
methods • Clot signature analysis(CSA) to assess PLT and clotting function • Pre- and post-OP venous blood were collected from 41 P’t of major orthopedic surgery