Download

1 / 7
0 likes | 3 Views
In the elbow, PRP injection for lateral epicondylitis can reduce pain with gripping, lifting, and computer work over several weeks.

E N D
Platelet rich plasma therapy moved from the training rooms of professional sports into mainstream clinics over the past decade, and for good reason. When done well, PRP joint injections harness a patient’s own biology to help nudge stubborn injuries toward healing. I have seen sprinters return from chronic tendinopathy without another course of anti- inflammatories, golfers cut down their shoulder pain enough to swing freely, and desk-bound patients ease knee osteoarthritis pain enough to keep up with their kids. PRP is not magic, and it does not cure everything, but it offers an option in that space between rest and surgery where many people get stuck. What PRP actually is A platelet rich plasma injection is made from your own blood. A clinician draws a small sample, typically 15 to 60 milliliters, then spins it in a centrifuge to separate the layers. The goal is to concentrate platelets, which carry growth factors and cytokines that signal cells to repair tissue. Platelet counts in PRP vary widely depending on equipment and technique. A good preparation yields platelet concentrations about 3 to 6 times baseline. Too low and you are essentially injecting dilute plasma. Too high and you risk platelet clumping and irritation. The sweet spot depends on the target tissue, the patient’s baseline platelet count, and the presence or absence of leukocytes. You will hear two terms in most clinics: leukocyte-rich PRP and leukocyte-poor PRP. Leukocytes are white blood cells. Leukocyte-rich formulations can be useful in chronic tendinitis where a controlled inflammatory push is desired. Leukocyte-poor PRP is often favored inside joints for knee osteoarthritis or cartilage damage where you want signaling without excess inflammatory debris. Both live under the umbrella of platelet rich plasma injections, and the specifics matter. How PRP injections work at the tissue level PRP treatment draws on the biology of normal wound healing. Platelets release growth factors such as PDGF, TGF-β, VEGF, and IGF-1 once they encounter collagen and are activated, either by contact with the injured tissue or by additives like calcium chloride. Those growth factors recruit reparative cells, stimulate collagen production, and encourage angiogenesis. In tendons, this translates to improved collagen alignment and strength over time. In joints, PRP therapy for joints can dampen inflammatory signals from the synovium, improve the viscoelastic properties of synovial fluid, and potentially protect cartilage cells. It is not “regrowing cartilage” in a dramatic sense, but some patients see meaningful symptom reduction and function gains that last months. Mechanism also explains variability. A PRP injection into a well-vascularized soft tissue behaves differently from a PRP knee injection bathing a degenerative joint. Technique, dosing, and timing change the outcome, which is why PRP injection therapy can look very different across clinics. Who tends to benefit Patterns emerge with experience. PRP joint injections most often help patients with: Mild to moderate knee osteoarthritis where pain flares with impact, stairs, or prolonged standing, and x-rays show joint space narrowing without end-stage bone-on-bone contact. Chronic tendinopathies that have resisted rest and basic rehab, such as PRP injection for tennis elbow, patellar tendinopathy, Achilles tendinopathy, or gluteal tendinopathy. Partial tears in tissue that has a fighting chance to remodel, like certain rotator cuff or hamstring injuries, and some ligament sprains. Focal cartilage issues like small chondral defects, or degenerative meniscus tears that remain symptomatic despite therapy. I also see PRP injection for shoulder arthritis improve night pain for some, and PRP injection for plantar fasciitis salvage runners who have cycled through orthotics, massage, and shockwave. PRP injection for wrist pain, ankle sprains, and elbow pain can move the needle when the diagnosis is clear and the rehab plan is disciplined. On the other hand, PRP injection for sciatica, PRP injection for herniated disc, or PRP injection for back pain in general lacks consistent evidence when injected into the spine or discs. Some clinics market injections for neck pain, but outcomes depend heavily on the exact source of pain. For spinal issues, I reserve PRP for very select cases or as part of a research protocol. The PRP injection procedure from start to finish
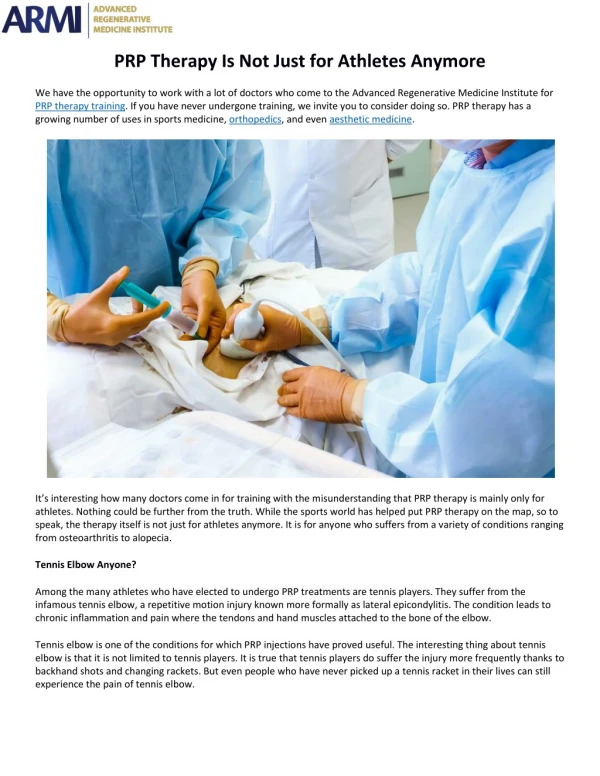
A typical PRP injection treatment takes 45 to 90 minutes. Patients usually stop non-steroidal anti-inflammatory drugs for several days before and after, since NSAIDs can blunt platelet signaling. Hydration helps, especially if you are prone to lightheadedness with blood draws. After consent and a focused exam, we draw blood from a vein in the arm and place it in centrifuge tubes. The spin takes about 5 to 15 minutes depending on the device. While the blood separates, we confirm the target with palpation and ultrasound. Ultrasound guidance improves accuracy, reduces the number of needle passes, and helps avoid structures you do not want to hit. If I am treating a knee, for example, I may direct the platelet rich plasma injection into the suprapatellar pouch and around the most inflamed synovial areas, or focus near a focal cartilage lesion. For a tendinopathy, I will often perform a gentle tenotomy, guiding the needle through the degenerated region to create microchannels that accept PRP and stimulate remodeling. Patients feel pressure and a deep ache during injection. The discomfort usually lasts a few minutes. For sensitive areas, we use local anesthesia on the skin and sometimes a small volume deeper, but avoid flooding the target with anesthetic because it can dilute PRP or affect platelet activation. After withdrawing the needle, we apply a small bandage. Most people walk out on their own. What to expect after PRP therapy The first 48 to 72 hours usually bring soreness, warmth, and stiffening. It can feel worse before it feels better. This early reaction is part of the inflammatory cascade that PRP triggers. Ice is fine in short bouts, but I prefer patients emphasize relative rest, gentle range of motion, and acetaminophen for pain. Avoid NSAIDs for one to two weeks if possible. If the joint swells, elevation and a compressive sleeve can help. Rehabilitation begins quickly with guided motion and progresses to targeted loading. With PRP injection for knees or hips, patients often settle into normal daily activity by day 3 to 7, then begin structured strengthening. For tendons, early isometrics can calm pain, followed by gradual eccentric loading. The cadence matters. Push too soon and you flare. Wait too long and you lose the remodeling window.
Improvement tends to appear in stages. Many patients note small wins by week 2 to 4, meaningful gains by week 6 to 8, and peak benefit around 3 months. PRP injection results last variable lengths of time. For knee osteoarthritis, responders often enjoy symptom relief for 6 to 12 months, sometimes longer. For tendons, the benefit can endure if the loading program continues and upstream biomechanical issues are addressed. Evidence, not hype The evidence base is not uniform. High-quality randomized trials support PRP knee injections in mild to moderate osteoarthritis, showing better symptom relief and function than saline and often better durability than hyaluronic acid injections. Compared with cortisone, PRP can lag in the first few weeks but pull ahead by 3 months and sustain improvements beyond 6 months in responders. PRP vs cortisone injection is a trade: steroids provide quick anti- inflammatory relief, but repeated shots can weaken tissue and provide diminishing returns. PRP asks for patience and pays off later. For lateral epicondylitis, or PRP injection for tennis elbow, multiple trials suggest PRP outperforms saline and sometimes dry needling at 6 to 12 months. For patellar and Achilles tendinopathy, outcomes vary, often tied to technique and rehab quality. Some studies show advantage, especially with ultrasound guidance and fenestration. Others show parity with well-structured exercise programs. That last point matters: PRP is not a shortcut around good rehabilitation. It is an adjunct. > Dr. V Medical Aesthetics Points of Interest POI Images TO Directions Iframe Embeds < Inside joints other than knees, evidence is emerging. PRP injection for shoulder osteoarthritis and for partial rotator cuff tears shows promise in symptom relief, particularly when combined with a shoulder-specific rehab plan. PRP local PRP injection services injection for ankle pain due to osteochondral lesions can help, often as part of a broader strategy including offloading and progressive loading.
Where the data do not support routine use: PRP injection for back pain, sciatica, or herniated discs as a general rule. Some niche applications exist, but patients should be wary of aggressive marketing that outpaces evidence. Technique, dosing, and why they matter When clinicians say PRP injection therapy, the phrase hides a lot of variables: platelet concentration, leukocyte content, activation method, volume, injection location, and number of treatments. A few practical lessons from clinic: Platelet concentration should usually fall between 3x and 6x baseline. Higher is not always better. Excessively high counts can be pro-inflammatory without added benefit. Leukocyte-poor PRP is often more comfortable inside joints. Leukocyte-rich PRP can be strategic in tendons that need a stronger inflammatory nudge. Ultrasound guidance reduces guesswork. Even experienced hands benefit from seeing the needle reach the target and distribute PRP where it matters. Volume matters. A small tendon might accept 2 to 4 milliliters, while a knee joint might benefit from 5 to 8 milliliters, sometimes more if multiple compartments are involved. Series vs single injection depends on condition and response. Many joints respond to one to two treatments spaced 4 to 6 weeks apart. Tough tendinopathies occasionally need a second pass if the first creates partial improvement without full resolution. This is why two patients can report different PRP injection reviews from two different clinics. The label is the same, the recipe is not. Safety profile and side effects Because PRP comes from your own blood, allergic reactions are rare. The most common side effects of PRP injection are temporary pain, swelling, and stiffness. Bruising at the blood draw site is common. Transient flares that last 2 to 7 days occur in a minority. Infection is possible but uncommon when sterile technique is observed. Nerve irritation can occur if a needle brushes a superficial nerve, usually resolving with time. Patients on blood thinners can still receive PRP, but bleeding risk and platelet function must be considered. Those with platelet disorders or very low baseline counts may not be good candidates. Active infection, uncontrolled diabetes, or poorly managed autoimmune conditions can complicate healing. For patients with severe joint deformity or bone-on- bone arthritis, PRP injection for degenerative joint disease may provide limited relief and should be framed as a bridge, not a cure. PRP vs other injections Patients often ask how PRP compares with steroid or hyaluronic acid. Cortisone is quick, inexpensive, and effective for short-term pain control. The downside is short duration and potential tissue weakening with repeated use. Hyaluronic acid aims to lubricate the joint and can help some knees for several months, but results vary and tend to be modest. PRP vs hyaluronic acid injection trials often favor PRP for longer-lasting function and pain improvements in mild to moderate osteoarthritis. PRP injection vs stem cell is not a fair match since “stem cell” therapies range from bone marrow aspirate concentrates to adipose-derived preparations and are regulated differently. Bone marrow aspirate contains a small number of progenitor cells along with cytokines. While some data suggest benefits, variability is wider, costs are higher, and regulatory oversight is stricter. In daily practice, I usually start with PRP for joints and tendons, escalate only when indicated, and discuss uncertainties candidly. Costs, logistics, and practical decisions Insurance coverage for platelet rich plasma therapy is inconsistent. Some plans cover PRP knee injections for osteoarthritis when other treatments fail. Many still consider PRP experimental and do not cover it. Out-of-pocket costs in the United States commonly range from a few hundred dollars to over a thousand per session, influenced by geography, clinic reputation, and whether multiple sites are treated in one visit. Ask about the preparation system, platelet counts, and whether the clinic uses ultrasound guidance. You should also clarify the expected number of treatments, the rehab plan, and follow-up schedule. A transparent clinic will discuss chances of success, likely PRP injection healing time, and what to do if you do not respond.
Where PRP fits in a full plan I rarely view PRP in isolation. The best results come when PRP injection for tendon repair is paired with targeted eccentric loading and return-to-sport progressions, or when PRP injection for cartilage repair coexists with strength training, weight management, and footwear changes. For knee osteoarthritis, even a 5 to 10 percent body weight reduction can take significant load off the joint, enhancing PRP’s effect. For runners, cadence adjustments and strength work often prevent the cycle that led to injury in the first place. Anecdotally, one of my marathon clients with persistent patellar tendinopathy plateaued with a well-executed program. He chose PRP, we did a leukocyte-rich preparation with ultrasound-guided fenestration, then resumed isometrics within three days, eccentrics by week two, and graduated to plyometrics by week six. His timeline to pain-free strides was 10 weeks. I contrast that with a recreational tennis player who expected a quick fix for lateral epicondylitis but skipped the progressive loading and kept playing through pain. Her PRP injection effectiveness was mediocre until we paused gripping-heavy drills and retrained forearm capacity. Biology needs cooperation. Addressing specific conditions people ask about PRP injection for rotator cuff issues: small partial-thickness tears and tendinopathy respond better than large full- thickness tears. Expect improved pain during overhead activity and better sleep if rehab is consistent. PRP injection for meniscus tear: degenerative tears can calm, particularly if mechanical symptoms are mild. Locking and catching suggest tears that might still need arthroscopy. PRP injection for ligament injury: grade 1 to 2 sprains in ankles and knees are good candidates, especially when the goal is to return to sport without lingering laxity. PRP injection for cartilage damage: focal lesions may benefit when offloading and strength are addressed. Symptom improvement is more reliable than structural regrowth. PRP injection for chronic tendinitis: consider it after 8 to 12 weeks of diligent loading work if pain and function plateau. Patients also ask about PRP for skin and hair. PRP injection for hair loss, PRP hair restoration, and PRP hair treatment have become common in dermatology, with sessions spaced a month apart for several rounds. Some people with androgenic alopecia notice thicker shafts and reduced shedding. For facial procedures such as PRP microneedling, PRP facial rejuvenation, or the so-called PRP vampire facial, the goal is collagen stimulation for texture and scar improvement. PRP injection for acne scars and under eyes can improve fine lines and dark circles in select cases. Those cosmetic applications are different in technique and expectation from PRP therapy for joints, but the biological rationale is similar. Results vary, and maintenance sessions are usually needed. How long PRP benefits last and when to repeat How long does PRP injection last? For joint pain, a pragmatic answer is 6 to 12 months in responders. Some repeat annually. For tendons, once healed, many remain well if they continue smart loading and avoid repeating the original error. If pain returns within a few months or never improves after 8 to 12 weeks, reconsider the diagnosis. Hidden drivers such as biomechanical deficits, training errors, or a different pain generator can sabotage results. The PRP injection success rate depends on condition and selection. In clinic, I counsel knee osteoarthritis patients that about 60 to 70 percent see meaningful improvement for several months, with better odds in milder disease. Tendinopathies respond well when ultrasound shows focal degeneration and the patient commits to rehab. Partial rotator cuff tears do better than massive tears. Numbers vary across studies, but that pattern holds. Risks, edge cases, and when to say no PRP injection risks are low, but honesty helps. I avoid PRP in the setting of uncontrolled inflammatory arthritis flare because it is hard to separate PRP-induced inflammation from a disease flare. I am cautious with smokers and those with poorly controlled diabetes, since microvascular compromise can blunt healing. For patients expecting to avoid knee replacement with PRP injection for degenerative joint disease when x-rays show severe narrowing and deformity, I refocus the conversation. PRP may soften pain temporarily, but mechanical problems persist. That money might be better saved for surgery or used for a targeted strengthening program and pain management. For athletes in season, timing is strategic. PRP injection for sports injuries can create a window of soreness. I plan injections around bye weeks or low-stakes periods. We pre-load the rehab plan so training volume resumes intelligently. Pain during and after: a realistic picture
PRP injection pain is usually brief during the procedure, described as pressure or burning. Afterward, many patients describe a deep ache that peaks in 24 to 48 hours and fades by day 3 to 7. For tendons, expect a sharper soreness at the needle track that transitions to stiffness. For joints, expect a heavy, full feeling. If pain escalates dramatically, if you spike a fever, or if the joint becomes red and hot, call your clinician. True infection is rare, but vigilance is wise. A simple comparison when choosing an injection Here is a concise way to think about your options if you and your clinician agree that an injection makes sense: Cortisone: quick relief, short duration, potential downsides with repeats. Hyaluronic acid: lubrication effect, moderate relief for some, variable. PRP: slower onset, potentially longer relief, biologically restorative signaling. Align the choice with your goals. If you need a short-term drop in pain to get through a specific event, a steroid might be the tool. If you want to reduce pain over months and invest in tissue quality with rehab, PRP deserves a look. What a good PRP program looks like I put the highest value on workflow and follow-through. The clinic draws sufficient blood, uses a validated centrifuge, documents platelet counts when possible, and selects leukocyte content based on target tissue. The clinician uses ultrasound for accuracy, minimizes anesthetic dilution, and injects the right volume in the right place. Post-procedure, there is a written plan: activity restrictions for the first 72 hours, pain control without NSAIDs, then a graded rehab schedule tied to tissue healing timelines. Follow-up visits check progress, not just pain scores but function, range of motion, and strength. Patients do their part by managing expectations and adhering to the plan. They ask about return-to-running timelines, when to resume heavy lifts, and how to taper back into sport. They report any abnormal swelling or fever. They understand that PRP injection effectiveness depends on both the biology in the syringe and the behavior after the visit. Answers to common practical questions How does PRP injection work? By concentrating platelets from your own blood and delivering them to an injured area to release growth factors that promote repair and modulate inflammation. What is PRP injection used for? Joint pain from osteoarthritis, tendinopathies, partial tendon or ligament injuries, and certain cartilage issues. There are also cosmetic and hair applications handled by dermatology and aesthetics. What is the PRP injection recovery time? Soreness for a few days, functional improvement over weeks, and peak benefit by 2 to 3 months in many musculoskeletal cases. What about PRP injection before and after? Photos make more sense for skin and hair. For joints and tendons, we track strength metrics, range, and validated pain scales rather than images. What is the PRP injection cost? Often several hundred to over a thousand dollars per session, with variable insurance coverage. Ask up front and avoid surprise bills. Are there alternatives? Yes. High-quality rehab, activity modification, bracing, shockwave for tendons, medications, and in some cases surgery. PRP vs steroid injection and PRP vs hyaluronic acid injection comparisons help frame the choice, but the broader plan matters most. A brief word on cosmetic PRP, then back to joints While this guide centers on PRP joint injections, many readers ask about PRP injection for skin rejuvenation, PRP facial injection, PRP injection for wrinkles, PRP injection for scar treatment, PRP injection for stretch marks, and PRP injection for under eyes. In aesthetics, clinicians combine PRP with microneedling or inject it directly in small volumes to stimulate collagen. Results can be subtle but real in the right candidates. PRP injection for hair growth, PRP scalp injections, and treatment for hair thinning or alopecia can reduce shedding and thicken hair shafts for some, usually over a series of treatments. If you pursue these, choose a clinic that sets realistic timelines, uses sterile technique, and offers maintenance plans without pressure.
Back to the musculoskeletal world, the through-line remains the same: clear diagnosis, targeted application, and disciplined follow-up. When PRP is worth considering If you are weighing PRP injection for knee osteoarthritis and you still have some joint space, remain active, and want to postpone or avoid surgery, PRP is reasonable. If you have a stubborn tendon that has not yielded to 8 to 12 weeks of thoughtful rehab, PRP could be the catalyst that restarts healing. If you want immediate pain relief for a short-term need, PRP may not fit your timeline. Ask the right questions. What formulation will be used? What does the clinic’s protocol look like for my diagnosis? How will we measure success? What is my PRP injection recovery time and return-to-activity plan? If the answers are precise, if ultrasound is routine, and if the rehab plan is specific, you are on firmer ground. PRP is a biologic nudge, not a miracle. It belongs in the same conversation as good coaching, smart loading, sleep, and honest timelines. For many athletes and patients, that combination is exactly what gets them back to doing what they love, with less pain and more confidence.