Download

1 / 6
0 likes | 1 Views
Cost and coverage for PRP injection vary, as it is often considered elective; clinics provide estimates and package options.

E N D
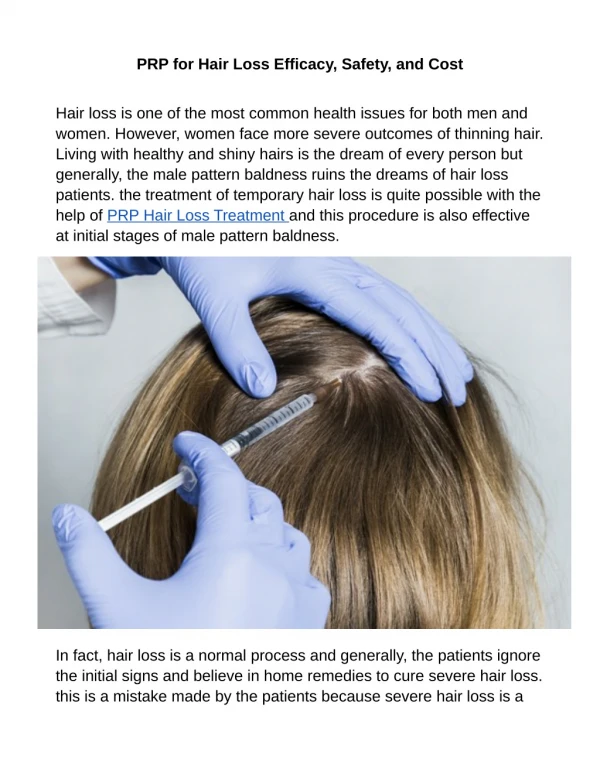
Platelet rich plasma has been the quiet workhorse of sports medicine for years, helping tendons and ligaments heal with fewer drugs and less downtime. When we brought PRP into hair restoration clinics, the logic was similar. Instead of transplanting hairs or flooding the scalp with medications, we concentrate your own platelets, return them to the thinning areas, and ask biology to do what it was designed to do: repair, stabilize, and nudge follicles back toward growth. I have used PRP injections alongside medical therapy and hair surgery for more than a decade. It is not a miracle, and it is not for everyone. Done well, though, it can slow shedding, thicken miniaturized hairs, and buy time before more invasive steps become necessary. The details matter. Candidate selection matters even more. What PRP actually is A PRP injection begins with your blood. We draw a small amount, usually between 10 and 60 milliliters depending on the system, then spin it in a centrifuge to separate the components. Red cells sink, platelets and plasma rise. The goal is to concentrate platelets well above baseline, most commonly in the range of 3x to 6x physiologic levels. That concentrate holds a dense cocktail of growth factors and cytokines, including PDGF, VEGF, TGF-beta, IGF-1, and EGF. These signaling molecules recruit healing cells, enhance blood vessel formation, and modulate inflammation. In hair, the targets are miniaturizing follicles stuck in a prolonged telogen or early catagen state. Androgenetic alopecia is the classic example. In that setting, platelet rich plasma injections appear to improve follicular microenvironment, increase dermal papilla activity, and prolong anagen. In plain language, the hairs spend more time growing and less time resting. This is distinct from PRP therapy for joints, where we inject around tendons, ligaments, or intra-articularly for knee osteoarthritis. Similar biology, different end goals. Who is a good candidate Not everyone who is shedding hair will benefit from PRP hair treatment. The best results I see follow a recognizable pattern: early to moderate thinning, intact miniaturized hairs on dermoscopy, and a scalp that still shows density when parted rather than islands of shiny baldness. Men in Norwood stages II to IV and women with Ludwig I to early II fit this profile. Once the scalp is smooth and reflective, follicles have scarred or disappeared, and PRP hair restoration has little to coax back. Age is less important than hair caliber and activity. I have treated a 26 year old with aggressive vertex thinning who responded beautifully because we caught miniaturization in flight, and a 58 year old postmenopausal woman whose crown filled in by roughly 15 percent after three sessions. On the other hand, a 35 year old with advanced bifrontal recession and slick temples saw almost no change. The follicles simply were not there to rescue. Underlying diagnoses matter. PRP scalp injections can help in traction alopecia if the pulling has stopped and follicles remain, but they do not reverse scarring alopecias like lichen planopilaris. Alopecia areata responds variably. Some small studies show benefit, particularly when disease is limited and quiet. In diffuse telogen effluvium triggered by illness or postpartum change, the hair will often recover without intervention. I counsel patience before any injection procedure in those cases. > Dr. V Medical Aesthetics Points of Interest POI Images TO Directions Iframe Embeds <
Medical history counts. If you take anticoagulants, have uncontrolled diabetes, significant anemia, platelet disorders, or active scalp infections, we either postpone or avoid PRP injection therapy. Smokers tend to respond less robustly. And if you are on isotretinoin or recently had a major inflammatory scalp event, we wait. A solid consult identifies these flags early and saves you time and money. How I set expectations The arc of benefit is gradual. During the first three months after PRP treatment injections, shedding usually decreases and hair feels grippier when you run hands through it. Between months three and six, we see an uptick in hair caliber and density on standardized photos or trichoscopy. After six to nine months, the curve plateaus. Maintenance sessions hold the gains. That is the typical course. There are exceptions, both faster and slower. What about numbers? In clinic, I see average terminal hair counts rise by 10 to 25 percent over baseline in good candidates after an induction series. Caliber increases 10 to 20 microns in many cases, which is more visible than it sounds. Shedding can drop by half. The literature varies, but those ranges are defensible. People often ask about PRP injection success rate. If success is defined as visibly thicker hair and less shedding on photography after a standard protocol, I estimate 60 to 70 percent for androgenetic patients chosen well. A smaller fraction, perhaps 10 to 15 percent, see impressive changes. Some see none. We try to identify the latter before starting. The session itself, step by step Clinicians differ in technique, but most share the same beats. You arrive without heavy hair products. We take photos from fixed angles with consistent lighting. I mark thinning zones with a dermographic pencil. A topical anesthetic can be used, though many prefer to avoid creams that might affect platelet function. Instead, I rely on nerve blocks with buffered lidocaine. Five quick injections numb the scalp lines most people feel. Clean the field. Draw blood. The blood goes into single or double spin centrifuges, depending on the kit. The difference matters. Double spin methods typically reach higher platelet concentrations and lower red cell contamination, though at the cost of time. I check the volume and opacity of the buffy coat, then harvest the platelet rich fraction. Some clinicians activate PRP with calcium chloride or thrombin just before injection. I reserve activation for certain indications, since premature degranulation may shorten the time growth factors remain at the follicle. For hair, nonactivated PRP generally performs well. Injection depth is shallow, in the dermis and superficial subdermis. I use a narrow gauge needle and a stamp-like pattern, spacing each microdeposit about one centimeter apart, adjusting depth and volume over denser or more affected zones. Total volume varies, but 3 to 8 milliliters is typical for a mid-sized scalp area. The PRP injection pain is tolerable after blocks. Without blocks, expect a sting and pressure that peaks over bony areas. The entire PRP injection procedure lasts 30 to 45 minutes once numb. Afterward, the scalp looks pink and slightly puffy. Tiny blebs flatten within an hour. I ask patients to avoid vigorous exercise, saunas, and hair dye for 24 to 48 hours, and to skip NSAIDs for three days. Tylenol is fine. You can wash hair that night or the next morning. How many sessions, and how often The schedule is one of the most common points of confusion, partly because different protocols circulate online. In practice, I favor an induction of three sessions, spaced four to six weeks apart, followed by maintenance every four to six months. That rhythm matches the hair cycle and balances biology with logistics. Some patients with brisk gains or high platelet concentrations can extend maintenance to eight or even 12 months. Others, especially those with fast-progressing hair loss, prefer quarterly touch-ups. A few clinics advertise a single large-volume PRP treatment with “booster” microneedling. I have not seen single-shot approaches outperform a series in androgenetic hair loss. Follicles respond to repeated nudges. The maintenance plan is not a scheme, it is physiology. What changes, and when you notice it Most people notice reduced shedding first. Showers are less dramatic, pillows less alarming. Then texture improves. The hair feels springier, less limp, and styles with less effort. Photos show tighter part lines and fewer scalp dots. This is the period where friends might say your hair looks healthy but cannot pinpoint why. Real density shifts, the kind that show
clearly on macro images, usually land between months three and six. They continue to build, then level out. If nothing obvious has changed by month four, we reassess, adjust the protocol, or stop. I had a patient in his early forties, prp injection Florida Norwood III vertex, whose job kept him under studio lights. He combined PRP therapy with topical minoxidil 5 percent foam nightly and low dose oral finasteride under medical supervision. Photos at week 12 showed a 14 percent increase in terminal hair count at the crown, and by month six he extended his haircut cycle from every three weeks to every five. That is a practical metric many people appreciate. Combining PRP with other treatments PRP pairs well with medical therapy. Finasteride or dutasteride aim at the hormonal driver in male and some female pattern loss, while minoxidil prolongs anagen. PRP improves the follicle’s environment. Together, they cover upstream and downstream. In women, we rule out iron deficiency, thyroid issues, and consider spironolactone when appropriate. Low level laser therapy can add a small boost for some. I am cautious about stacking too many interventions at once, because it muddles attribution. We introduce changes deliberately. O-Shot Gonzalez FL - Dr. V Medical Aesthetics - 850-724-08 O-Shot Gonzalez FL - Dr. V Medical Aesthetics - 850-724-08… … If you are planning hair transplant surgery, PRP can support both donor and recipient healing. I often perform a PRP injection treatment at the time of grafting and another at three to four months. It appears to accelerate graft growth and may decrease shock loss of surrounding native hairs. Again, expectations must be realistic. PRP is supportive, not substitutional, for areas that are severely depleted. Safety, side effects, and risks Because PRP uses your own blood, allergic reactions are rare. That does not mean risk-free. Common post treatment sensations include tenderness, swelling, mild bruising at injection sites, and headache that resolves within a day. A transient flare of shedding sometimes follows the first session, likely from synchronization of follicles. It passes. Infection is possible whenever needles enter the skin, so sterile technique is nonnegotiable. I have seen two cases of folliculitis after scalp PRP, both resolved with topical antibiotics. Scar risk is minimal with proper technique. Nerve irritation can cause temporary numb patches when injections get too deep near the temporal lines. If you bruise easily or take blood thinners, bruising will be more pronounced, and we discuss that beforehand. The kit and technique influence risk. Avoid clinics that cannot describe their protocol, do not photograph outcomes, or promise guaranteed results. A platelet rich plasma injection should not contain visible red streaks or foam. If you see that in the syringe, it suggests contamination with red cells or air, which can increase inflammation or compromise comfort. Cost and value Prices vary widely by region and clinic experience. In the United States, a single PRP hair session typically ranges from 500 to 1,500 dollars. Package pricing for an induction series may provide some savings. I advise people to calculate the yearly cost including maintenance rather than fixating on the first visit. Compare that to the cost of medical therapy, laser
devices, or delaying transplant. Value hinges on candidacy and response. If your first two sessions show no change in shedding, texture, or photo metrics, it may be wiser to stop rather than chase sunk costs. How PRP compares to other injections Patients often ask how PRP injection vs steroid injection or hyaluronic acid shakes out. Steroids calm inflammation, useful for inflammatory scalp conditions but not helpful, and potentially harmful, in androgenetic thinning where they can worsen atrophy if misused. Hyaluronic acid injections add volume in joints, and in aesthetics hydrate tissue, but they do not promote hair growth. PRP vs cortisone injection in joints is a different conversation. For knee osteoarthritis, PRP knee injections often provide longer symptom relief than corticosteroids, with fewer long term downsides, though results depend on disease stage. For tendons, PRP injection for tendinitis and PRP injection for tennis elbow have reasonable evidence in chronic cases that failed conservative care. Those same biological principles lend plausibility to scalp applications, but the end points differ. People also ask about PRP injection vs stem cell therapies. True stem cell treatments remain experimental and heavily regulated. Many clinics advertise “stem cells” when they mean stromal vascular fraction or amniotic products with variable contents. Platelet rich plasma therapy is autologous, relatively simple, and better studied than most so-called regenerative products marketed for hair. Technique details that change outcomes The devil is in the technical decisions. Platelet concentration that is too low behaves like plasma. Too high, above roughly 7x to 8x baseline in some studies, may inhibit follicular cells due to excessive growth factor levels. The sweet spot varies by kit and patient. Leucocyte content matters. Leukocyte-rich PRP can be more inflammatory, which helps in tendons but might irritate scalp tissue. I favor leukocyte-poor PRP for hair. Activation timing changes release kinetics. Nonactivated PRP releases growth factors as platelets encounter collagen and thrombin in the scalp, spreading the effect over hours to days. Activated PRP releases more immediately. Needle size and spacing affect comfort and distribution. Even the direction of injection matters over the frontal hairline to avoid vascular compromise. These are not minor points, and they separate competent PRP injection treatment from haphazard efforts. What to do before and after sessions A few preparatory and aftercare choices make a difference. Hydrate well for 24 hours before your appointment, and eat a small meal. It makes the blood draw smoother and reduces lightheadedness. Pause NSAIDs such as ibuprofen for three days before and after if your doctor agrees, since they can blunt platelet function. Avoid hair dye, harsh scalp treatments, and spray tans for 48 hours before and after, to reduce irritation and contamination risk. Sleep with your head slightly elevated the first night if you tend to swell, and use a clean pillowcase. Book follow-up photos and assessments at consistent intervals and lighting. Memory lies. Images help make good decisions. That is the only list I hand out. The rest is straightforward common sense and a short window of caution. The edge cases worth discussing Diffuse thinning in women can be a puzzle. Ferritin under about 50 to 70 ng/mL correlates with extra shedding even when still technically normal. In those women, PRP will underperform until iron is repleted. In men with low baseline platelet counts or significant smoking history, responses tend to be blunted. Autoimmune disease is not an absolute contraindication, but if the scalp Extra resources shows active inflammatory signs, I address that first. If you are on anticoagulation that you cannot pause, we discuss the bleeding risk and might defer. There is also the psychology of hair loss. People often come to PRP therapy after trying supplements and shampoos that promised too much. They feel burned. The last thing they need is more magical thinking. I anchor our plan to measurable endpoints: hair counts on a 1 cm square, hair caliber by dermoscopy, standardized photos, and patient-reported shedding scales. If we do not move the needle, we stop. How long results last
PRP injection results are not permanent in the sense of a cure. Androgenetic alopecia is a chronic process. Think of PRP as shifting the balance toward growth and health for a period, then reinforcing it at intervals. With maintenance, many hold improved density for years. Without it, hair tends to drift back to its pre-treatment trajectory over 12 to 18 months. The slope varies. Younger patients with earlier disease often hold gains longer. People with faster-moving hair loss lose them sooner. Frequently asked practical questions How much does it hurt? With proper nerve blocks, patients rate PRP injection pain between 2 and 4 out of 10. Without blocks, more like 5 to 7 over sensitive zones. Will I be presentable after? Yes. Expect mild redness and pinpoint marks that settle quickly. Most return to work the same day. Can I work out? Give it 24 hours. Heavy sweating and vasodilation can worsen swelling. Can I combine with microneedling? Yes, but timing matters. Some clinics perform PRP microneedling as a surface treatment. I prefer intradermal injections for depth control. Surface needling can be added conservatively for scalp health, but it is not a substitute for injections. Does PRP help scars? Platelet rich plasma treatment can improve scar texture and healing in skin. For acne scars, PRP facial injection or PRP microneedling has a role. That is a different protocol than the scalp, with its own expectations. What good looks like, and what to avoid A reliable clinic will take a proper history, examine your scalp with trichoscopy, photograph methodically, explain the PRP injection procedure, and discuss costs without pressure. They should talk through risks, alternatives like medical therapy and transplant, and what outcomes look like if you do nothing. Be wary of anyone promising guaranteed hair growth, or using buzzwords without specifics. Ask what their PRP preparation is, how many platelets it yields, whether it is leukocyte-poor or rich, how many sessions they recommend, and how they measure outcomes. If they cannot answer, keep looking. Where PRP fits in the broader landscape Hair restoration sits on three pillars: medical therapy to slow loss, procedural therapy to thicken what you have, and surgical therapy to redistribute hair from areas of abundance to areas of need. Platelet rich plasma injection therapy is procedural. It is not a replacement for finasteride in men or a full transplant in advanced cases. It is part of a thoughtful plan. I have patients for whom PRP hair treatment delayed transplant for several years. I have others who used PRP to stabilize while they tapered off oral medications due to side effects. For some, PRP joint injections made their knees comfortable enough to stick with exercise, which in turn improved metabolic health and hair. Biology is not siloed. We treat people, not just scalps.
Final thoughts from the chair PRP injection for hair loss sits in a practical middle ground. It harnesses your own biology, carries a modest side effect profile, and can produce visible, meaningful improvements when you catch hair loss at the right time. The trade-offs are cost, the need for repeated sessions, and the reality that not everyone responds. If you are considering it, get an honest assessment, commit to a series rather than a single test shot, and pair it with sensible medical therapy when appropriate. Measure your progress. Treat other contributors like iron deficiency or thyroid imbalance. Give biology a fair chance to help you, then hold it accountable. That balance of optimism and rigor is where PRP therapy earns its place.