Download
1 / 25
300 likes | 821 Views
Pharmacokinetics in drug design. Pharmacokinetics is how a drug is A bsorbed, M etabolized, D istributed, and E liminated. (ADME)…. Most drugs are given orally: dissolves in the GI tract and is absorbed through the gut; passes through the liver and into the blood stream.

E N D
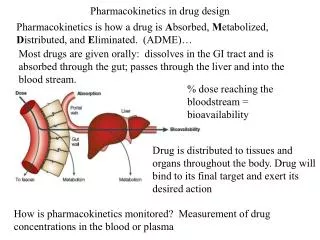
Pharmacokinetics in drug design Pharmacokinetics is how a drug is Absorbed, Metabolized, Distributed, and Eliminated. (ADME)… Most drugs are given orally: dissolves in the GI tract and is absorbed through the gut; passes through the liver and into the blood stream. % dose reaching the bloodstream = bioavailability Drug is distributed to tissues and organs throughout the body. Drug will bind to its final target and exert its desired action How is pharmacokinetics monitored? Measurement of drug concentrations in the blood or plasma
Pharmacokinetics in drug design Vd = apparent volume of distribution total blood volume = 5L in a 70kg person; 0.071L/kg
Pharmacokinetics in drug design Pharmacokinetics influences the required dosage:
Pharmacokinetics in drug design • A drug’s success in reaching the target depends on its physical • and chemical properties • 1. Chemical stability • Does it decompose in aqueous solution? • Does it survive stomach acid? Must it be injected? • 2. Metabolic stability • It must survive digestive and metabolic enzymes (liver) • Any metabolites (product of drug metabolism) should not be toxic or lose activity • Metabolic enzyme activity (cyctochrome P450’s) • varies from individual to individual • can be affected by other chemicals (grapefruit juice inhibits activity; cigarette smoke and brussel sprouts enhance it; other drugs may inhibit or promote P450 enzymes = drug-drug interactions).
2. Metabolic stability (continued) Drug - drug interaction examples: • Antibiotics can act as P450 inhibitors; slows the metabolism of other drugs by these enzymes. • Phenobarbitone (barbituate) stimulates the P450 enzymes, accelerating the metabolism of Warfarin (anticoagulant), making it less effective. • Cimetidine (antihistamine) inhibits the P450 enzymes, slowing the metabolism of Warfarin (anticoagulant). • St. John’s wort (herbal medicine for mild to moderate depression) promotes P450 enzymes, decreasing the effectiveness of contraceptives and warfarin. • Anticoagulants are bound by plasma protein in the blood, but aspirin displaces them, which can lead to a drug overdose.
3. Successful Absorption • Diffusion across membrane (solubility and permeability; size, H-bonding) • Transporters Too hydrophilic: cant cross membranes; more easily excreted by kidneys Too hydrophobic: poor water solubility, poorly absorbed from GI tract because they coagulate in fatty globules. Strategies to address hydrophilic/hydrophobic balance: a. Use of amines with pKa = 6-8. If pKa is out of range, change the structure of the amine to change the pKa. (2° to 3°; change substituents on an aryl amine) pKa = -logKa b. Inject into blood supply (bypass the gut)
c. Take advantage of carrier proteins in cell membranes that transport sugars, amino acids, neurotransmitters, and metal ions. If drug resembles these, maybe the drug can be transported across membranes. • Examples of use of carrier proteins to deliver drugs: • Levodopa (prodrug - later) is transported by phenylalanine transporter • Fluorouracil is transported by thymine and uracil transporters • Lisinopril (antihypertensive) is transported by dipeptide transporters.
d. Use of medicinal chemistry to improve hydrophobic/hydrophilic balance. • Change functional groups: Alcohol (ROH) versus ether (ROR’) or ester (RO2R’) • Change the number or size of alkyl groups • Change rings • Example:
Pharmacokinetics in drug design Return to 2. Metabolic stability: • Metabolism of drugs occurs in liver, kidneys, intestine, lungs, blood and skin, mostly catalyzed by enzymes. • Generally, metabolic products are more water soluble than starting compounds, so they may be readily excreted. • Phase I Metabolic reactions include oxidations (cytochrome P450 enzymes, flavin monooxygenase, others), reductions, and hydrolyses • Phase II metabolic reactions are the conjugation of metabolic products to other small molecules via carboxyl, hydroxyl, thiol, and amino groups. Conjugated products are even MORE water soluble than the metabolites, have no toxicity or pharmacological activity Examples of Phase I reactions on following slides...
Phase II: conjugation reactions Metabolism of Aspirin:
Strategies to make drugs more resistant to hydrolysis and metabolism, prolonging activity. A. Steric “shields” to prevent the approach of a nucleophile or enzyme to a susceptible group on the drug: B. Isosteric/bioisosteric replacement: change an ester (more reactive) to amide (less reactive)
C. Both effects: Procaine is a short-lasting anaesthetic because of ester hydrolysis How is lidocaine protected from hydrolysis?
C. Both effects: Procaine is a short-lasting anaesthetic because of ester hydrolysis How is lidocaine protected from hydrolysis? Steric shielding - methyl groups on phenyl ring Ester has been changed to less reactive amide
Strategies to make drugs more resistant to metabolic enzymes Removal of functional groups that are susceptible to metabolic enzymes. (aryl methyl groups are oxidized to carboxylic acids and eliminated from the body; C-hydroxylations; N and S oxidations, O and S dealkylations, and deamination). Strategies to make drugs less resistant to metabolic enzymes If a drug is too resistant to metabolism, it can pose problems as well (toxicity, long-lasting side effects). Add functional groups that are susceptible to metabolic enzymes: Ex. Anti-asthmatic drugs
Prodrugs are useful approach to overcome MANY types of problems Prodrugs are compounds that are inactive, but are converted in the body to an active drug using the body’s metabolic enzymes! A. Prodrugs to improve membrane permeability 1. Esters. If a carboxylic acid is important for drug binding to its target, but it prevents the drug from crossing a membrane, temporarily “hide” it as an ester. Once in the blood, it is hydrolized to the active form by esterases in the blood.
2. N-methylation. Since N-demethylation is a common liver metabolic reaction, amines may be methylated to increase hydrophobicity. These N-methyl groups will be removed in the liver. 3. Take advantage of membrane transporter. Ex. Parkinson’s disease is due to a deficiency of dopamine.
B. Prodrugs to prolong drug activity 6-mercaptopurine is used to suppress the immune system (organ transplants), but is eliminated from the body quickly. A prodrug that slowly is converted to the drug allows a sustained activity. C. Prodrugs to mask toxicity and/or side effects. 1. Salicylic acid is a painkiller, but phenolic -OH causes gastric bleeding. Aspirin has an ester to mask this toxic group until it is hydrolyzed
2. Antiviral drugs (AZT, acyclovir). Nontoxic until they are converted to toxic triphosphates by viral enzymes in infected cells. These phosphorylated compounds are both competetive inhibitors and chain terminators:
Pharmacokinetics in drug design Want to be able to look at molecular properties and predict ADME! • Log P: water-octanol partition coefficient • Solubility: turbidity • pKa: • Artificial membrane permeability • Binding to liposomes (SPR) • Presence of functional groups to predict metabolic products
References Patrick, G. L. An Introduction to Medicinal Chemistry; Oxford University Press: New York, NY, 2001 Van de Waterbeemd, H.; Gifford, E. “ADMET in silico modelling: towards prediction paradise?” Nat. Rev. Drug Disc., 2003, 2, 192-204.