Download
1 / 23
240 likes | 536 Views
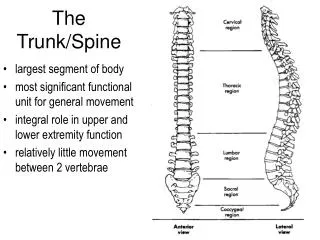
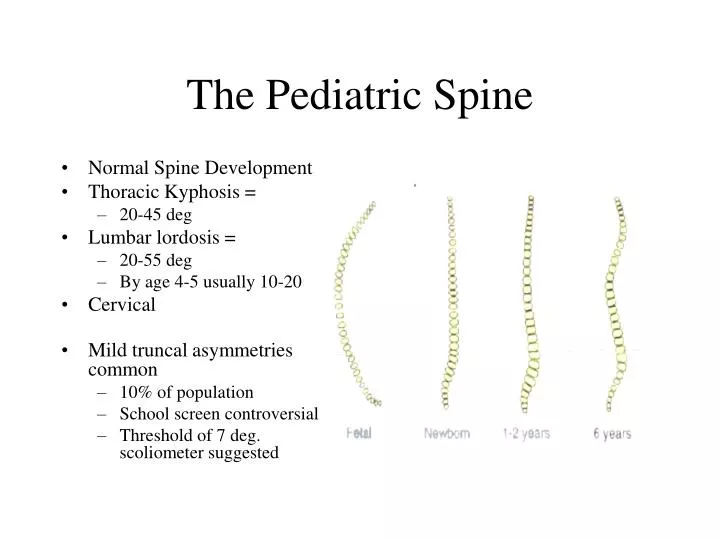
Normal Spine Development Thoracic Kyphosis = 20-45 deg Lumbar lordosis = 20-55 deg By age 4-5 usually 10-20 Cervical Mild truncal asymmetries common 10% of population School screen controversial Threshold of 7 deg. scoliometer suggested. The Pediatric Spine.

E N D
Normal Spine Development Thoracic Kyphosis = 20-45 deg Lumbar lordosis = 20-55 deg By age 4-5 usually 10-20 Cervical Mild truncal asymmetries common 10% of population School screen controversial Threshold of 7 deg. scoliometer suggested The Pediatric Spine
Spinal Flexion and Extension • Cerebral Palsy • Tightness: • Cervical and capital flexion • Thoracic extension • Lateral flexion • Lumbar flexion
Kyphosis • Postural • Congenital • Failure of formation and/or segmentation • Apex of curve between T10 and L1 most common • Failure of formation lead to paraplegia • Progressive under 55-60 deg. – post. Fusion • More than 60 deg – ant. and post.
Familial disorder of thoracic spine Hx of heavy physical loading from work or athletics Vertebral wedging and kyphosis >45 deg <60 – encourage activity >60 - brace Mild scoliosis Tx: NSAIDs, rest, stress reduction, TSLO for pain Scheurermann Disease
Variations common in typical prepubescent child Functional Compensation for fixed deformity above or below LS level Structural hyper/hypo Arrest growth of post lumbar vert with shunting or rhizotomy Muscular dsytrophy = hypo Fractures = hypo or hyper Lordosis
Cervical Problems • Basilar impression • Congenital or acquired • Cervical spine extends into the formamen magnum • May be due to osteopenia: • rickets • osteogenesis imperfecta
Occipital-atlantal instability • Rare but sometimes in Down Syndrome • Atlantoaxial instability • Due to abnormalities of odontoid or to ligamentous laxity • Down Syndrome, Rheummatoid arthritis, • Sx: gait disturbance, ex. Intolerance, neck pain • Mild weakness and hyperreflexia • Avoid cervical spine stress
Can have instability until the epiphysis closes X-rays recommended at age 2 y.r. in the case of Down Syndrome Case example: 7 year old high functioning child with Down Syndrome, in a regular classroom who can ride a tricycle independently. He/she falls off and becomes a paraplegic due to an unstable AA joint
Progression of scoliosis Chiari malformation Tethered cord Tumors Unresolved torticollis Clumsiness UE weakness Neurological Abnormalities
Abnormal skin lesions in midline Dimples Hemangiomas Hair patches Cavus feet Leg atrophy Café au lait spots
Back Pain • Referral important if • Onset before age 4 years • Symptoms persist longer than 4 weeks or increases • Pain interferes with function • Recent onset of scoliosis • Evaluate for: • Mobility and symmetry • Tenderness • Neurological signs – especially asymmetry
Spondylolysis and Spondylolisthesis • (B) or unilat defects of pars interarticularis = Sphondylolysis • 4% of 4 yo, 6% by maturity • If this displaces = spondylolisthesis • Most common form of back pain in children and adults and in children with abnormal bone or connective tissue • Usually due to stress fracture • Tenderness over L5-S1 • Limited SLR and forward bending • Pain aggravated by activity, especially competitive sports • Usually pain decreases as child becomes an adult due to decreased activity
Benign Back Pain in Children and Adolescents over ½ in this category Limit back pack weight (< 20% of body wt Not EBP Encourage healthy lifestyle, activity, weight reduction Disc Herniation Rare unless family hx, recent trauma, facet asymmetry, spinal stenosis, transitional vertebrae and spondylolisthesis Usually L4-5 or L5-S1 with radicular pain and secondary spinal deformity Tx: NSAID, rest, limited activity, TLSO MR and disc excision if persists
Unknown origin Most common Infantile: birth to 3 yrs Juvenile: 3-10 yrs Adolescent: >10 yrs Prevalence: 2-3% for curves <10 deg .2 to .3% for curves >20 deg Idiopathic Scoliosis
Correct on lateral trunk bending Causes: Pelvic Obliquity LLD Tumor Muscle spasm Fixed and do not correct Rotary component present and visible with forward bending Primary and compensatory curves Nonstructural and Structural
Neurofibromatosis • Mutation of neurofibromatosis (Type 1) or schwannomin (Type 2) gene • Type 2 has fewer peripheral but more intracranilal lesions • Scoliosis is idiopathic or dystropic • Dystropic involves short and sharp angulation and spinal instability • Fusion is indicated because of risk of boney dysplasia
School Screenings • Examine posture anteriorly and posteriorly • Forward bend test • MD and RN do this and often miss some cases • Assess for asymmetries: • Shoulders, nipple, scapula, pelvic heights • Asymmetrical folds of trunk • Curvature of spine
Treatment for Scoliosis • Young adolescents prepuberty will most likely progress • Curves <25 deg: observe • Curves 25-40 deg: non-surgical methods • Goal is to maintain with exercise and brace • TLSO 18-23 hours per day until skeletal maturity • PT: donning orthosis, schedule, skin care, exercise for ROM (hip flexors) and strength (abdom, gluts, paraspinals) • Curves >40 deg: surgical intervention
Surgery for Scoliosis • Indications: • Curve >40 deg • Curve is progressing • Decompensation of spine or thoracic cavity • Instrumentation: • Distract and compress the curve • Correct or minimize the rotory component • Stabilize and maintain • Harrington rods • PT: • Preop and postop for ROM, trunk strengthening, deep breathing and coughing • Early transfers and gait