Download
1 / 27
270 likes | 294 Views
Module: Health Psychology Lecture: Health Behaviours and Beliefs Date: 26 January 2009. Chris Bridle, PhD, CPsychol Associate Professor (Reader) Warwick Medical School University of Warwick Tel: +44(24) 761 50222 Email: C.Bridle@warwick.ac.uk www.warwick.ac.uk/go/hpsych.

E N D
Module: Health PsychologyLecture: Health Behaviours and BeliefsDate: 26 January 2009 Chris Bridle, PhD, CPsychol Associate Professor (Reader) Warwick Medical School University of Warwick Tel: +44(24) 761 50222 Email: C.Bridle@warwick.ac.ukwww.warwick.ac.uk/go/hpsych
Aims and Objectives • Aim: To provide an overview of the psychological determinants of health-related behaviours and beliefs • Objectives: The student should be able to provide a basic description of the … • meaning of health-related behaviours, and provide examples of different types of health behaviour • psychological processes that influence health behaviours and a framework for their organisation • common psychological components of health behaviour theories • core constructs relevant to understanding, predicting and changing health-related behaviours
Dual Pathway: Psychology and Health Psychological Factors Physical Health Direct Path Indirect Path Health Behaviour What psychological processes transmit influence along these paths?
Recap • Psychoneuroimmunology (PNI) • Physiological reactivity = mechanism of action • Stress & negative affect = influence being transmitted • Interpretation = process generating the influence • Negative physical effects = chronic stable exposure
Dual Pathway: Psychology and Health Psychological Factors Involved In Appraisal Physical Health: Physiological Reactivity Chronic Stress& Negative Affect Indirect Path Stable individual differences Health Behaviour Which stable factors, and what else?
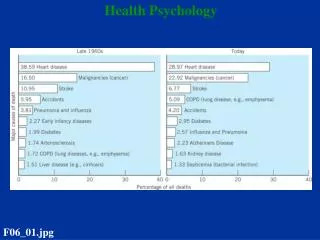
Q: Why focus on the indirect behavioural route? Leading Causes of Disease 20% 20% 50% 10% Behavioural contribution to management of chronic illness estimated at >90% (Wanless, 2004) (Healthy People 2000)
Key Questions • What psychological factors influence health behaviour? • What do we know about the determinants of health behaviour? • To what extent are we able to sufficiently explain and predict health behaviour? • Can our understanding of psychological processes be used to change health behaviour? • Will interventions that change health behaviour yield benefits for physical health?
Defining Behaviour • Behaviour: the actions or reactions of an individual to a situation – can be conscious or unconscious, voluntary or involuntary • But … what specifically? Health behaviour Illness behaviour Adaptive behaviour Maladaptive behaviour Prevention behaviour Detection behaviour Public behaviour Private behaviour Service-use behaviours Self-care behaviours Health behaviour: Behaviour that may have implications for health
Determinants of Health Behaviour A framework • Background factors: Characteristics that define the context in which people live their lives; shared understanding and ways of knowing the world • Stable factors: Individual differences (personality) in psychological activity that are stable over time and context • Social factors: Social connections in the immediate environment; mostly stable, but can be fragile, e.g. when in conflict with background factors • Situational factors: Appraisal of personal relevance that shape responses in a specific situation
Why a Framework? Background factors Stable factors Social factors Situational factors Distal Proximal Different intervention targets require different intervention strategies We bring with us, to any situation, the cumulative influence of background, stable and social factors, which we combine in various ways to form an understanding of our current situation. In most cases, our understanding (appraisal) of the situation determines our behaviour within it.
Stable Factors • Stable factors: i.e. individual differences, dispositions, personality • Refer to variations, between people, in psychological activities that, within people, produce responses that are stable across time and context • Influence appraisal in three key ways: • they determine if, and to what extent, an event is salient, i.e. sensitivity towards particular types of event • they provide a generalised framework for understanding and evaluating the event, e.g. as threat or challenge • they make available, or suggest, potential responses, i.e. initial response options
Individual Differences and Health Temporal dimension: Present Future Past • Three broad types of individual differences: • Emotional dispositions: Psychological processes involved in both the experience and expression • Generalised expectancies: Psychological processes involved in formulating expectations in relation to future outcomes • Explanatory styles: Psychological processes involved in explaining the causes of negative events
Emotional Dispositions • Negative affect: Tendency toward the experience of negative affective states, e.g. hostility, depression, anxiety • Appraisal bias for heightened arousal and increased frequency • Evidence for causal role in development of physical disease - health behaviour impeded as a function of fatigue and apathy. • Emotional expression: The (low) expression of (negative) emotional experience, both unconscious repression and conscious suppression • Appraisal bias for neutralising threat or extreme intensity, both leading to maladaptive responses • Risk factor for recovery (post-MI) and cancer progression
Generalised Expectancies • Locus of control: Expectations that future outcomes will be determined by factors that are either internal (self) or external (powerful others, and chance) • Internal loci generally associated with more favourable outcomes, and performance of health behaviours, but VERY dependent situational factors • Self-efficacy: Belief in one’s own ability to organise and execute a course of action, and the expectation that the action will result in, or lead to, a desired outcome • Heuristic belief in the beneficial effects of higher self-efficacy, deriving from appraisal bias for challenge rather than threat and expectation of success
Explanatory Styles • Optimism (Pessimism): Expectation of positive future outcome (however achieved) despite current negative event • Appraisal bias for brief, low levels of physiological reactivity, and promoting active coping responses • Optimism, vis-à-vis pessimism, associated with better physical health, illness recovery, and health behaviour performance • Attributional style: Causal explanations of negative events as internal (self), stabile (time), and global (situation) • Generally better if attributions are external, unstable and specific, rather than internal, stable and global • Causal attributions influence expectations about controllability of future outcomes, i.e. the relevance of health behaviours
Social Cognition Theories • Social cognition theories attempt to explain the relationship between social cognitions (e.g. beliefs, attitudes, goals, etc.) and behaviour • Some examples: • Health Belief Model (Rosenstock, 1966) • Protection Motivation Theory (Rogers, 1975) • Theory of Reasoned Action (Fishbein & Ajzen, 1975) • Theory of Planned Behaviour (Ajzen, 1988) • Transtheoretical Model (Prochaska and DiClemente, 1983)
Health-Belief Model (HBM) Perceived Susceptibility Perceived Threat Perceived Severity Health Behaviour Perceived Benefits Perceived Efficacy Perceived Barriers (Rosenstock, 1966)
Theory of Planned Behaviour (TPB) Behavioural beliefs + Outcome evaluation Behavioural Attitude Normative beliefs + Motivation to comply Subjective Norm Behavioural Intention Behaviour Control beliefs + Self-efficacy Perceived Behavioural Control (Ajzen, 1988)
(Prochaska & DiClemente, 1983) Transtheoretical Model Experiential + Processes of Change + Behavioural Stages of Change PC C P A M Self-Efficacy Temptations Pros Cons
Health Behaviour Models / Theories • Which model / theory is best? • At the end of every ‘theory’ chapter in every health psychology text, you’ll receive the following expert advice: ‘Models are not in competition … … they offer different perspectives on the relationship between social cognitions and (health) behaviour … …’ … blar, blar, blar, blar …
Which ‘perspectives’, on which ‘relationships’ and between what cognitions, etc., will help us to … understand … … predict …. … and change … … the health damaging behaviours in which so many people habitually engage?
Conceptual Framework • Determinants of health behaviours and beliefs • Background factors: Cultural norms; SES; Gender; Ethnicity; Genes; Chronic health status • Stable factors:Emotional disposition, Generalised expectancies; Explanatory styles • Social factors:Perceived support (family, friends, peers, etc.); Subjective norm; Helping relationships • Situational factors: Situation-specific self-efficacy; Perceived risk; Emotional response; Intention (motivation); Outcome evaluation;
Conclusions • There are many determinants of health-related behaviours • Determinants can be usefully grouped to form a conceptual framework • Background, stable and social factors shape beliefs and situational appraisals • Behaviour (typically) is most strongly influenced by situational beliefs / appraisals • Psychological models attempt to explain the relationship between beliefs and behaviour • Changing beliefs promotes long-term behaviour change
Summary • This session would have helped the student to understand the … • range of behaviours that can be described as being health-related • different types of determinants of health-related behaviours and the level at which they operate • common psychological components of health behaviour theories • core constructs relevant to understanding, predicting and changing health-related behaviours
Next Week • Illness Behaviours & Beliefs • Common sense would suggest that people who seek medical help have more severe symptoms than those who do not seek help. • Research demonstrates that this is incorrect. • Peoples interpretation of their symptoms and their help-seeking behaviour is determined by many factors aside from the presence or severity of physical symptoms. • These factors will be the examined in next week’s session.
Any questions? • What now? • Obtain / download one of the recommended readings • In your small groups consider today’s lecture in relation to next week’s tutorial tasks: a) integrated template b) ESA question