Case Report
Radiological Category:. Pediatrics. Principal Modality (1): Principal Modality (2):. CT. none. Case Report . Submitted by:. Alaina Moore, MSIV. Faculty reviewer:. Sandra Oldham, M.D. Date accepted:. 24 August 2010. Case History.


Case Report
E N D
Presentation Transcript
Radiological Category: Pediatrics Principal Modality (1): Principal Modality (2): CT none Case Report Submitted by: Alaina Moore, MSIV Faculty reviewer: Sandra Oldham, M.D Date accepted: 24 August 2010
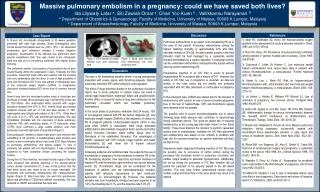
Case History 11 year old female is referred from ENT for outpatient CT to evaluate soft tissue nodule of neck. About 9 months prior, she presented to the ER with a painful nodule in the neck and was sent home with antibiotics. No other medical history is available.
Test Your Diagnosis Which one of the following is your choice for the appropriate diagnosis? After your selection, go to next page. • Ectopic thyroid • Thyroglossal duct cyst • Dermoid cyst • Lymphadenopathy • Cystic hygroma • Abscess • Branchial cleft cyst • Thymic cyst
There is a well-circumscribed, anterior, midline cyst that lies inferior to the hyoid bone and anterosuperior to the isthmus of the thyroid gland. It is of low density at approximately 25 HU and measures 20 mm x 7 mm x 15 mm. It appears to be separate from the thyroid gland. There are no calcifications, other masses, or inflammatory changes.There is tonsillar hypertrophy. The airway is patent, the vascular structures are normal, and there are no bony abnormalities. Findings and Differentials Findings: Differentials: • Thyroglossal duct cyst • Ectopic thyroid • Dermoid cyst • Branchial cleft cyst • Cystic hygroma • Thymic cyst
Thyroglossal Duct Cyst The thyroid gland begins development in third week of gestation as an outgrowth from floor of pharynx at the foramen cecum. It descends through the neck, passing anterior to the developing hyoid bone. It should reach the inferior neck by the seventh week gestation. This primordial thyroid remains connected to the tongue by the thyroglossal duct. Involution usually occurs by the tenth week gestation. The distal end of the duct can become the pyramidal lobe of the thyroid. If a portion of the duct persists, secretion from the epithelial lining can form a cyst. Thyroglossal duct cyst accounts for 70% of congenital neck anomalies. 75% are midline in location 80% are at the level of or inferior to the hyoid bone The clinical presentation is usually of a gradually enlarging, painless, midline neck mass in children and young adults which moves upward with tongue protrusion. Cyst is often discovered when it becomes infected. Discussion
Imaging Ultrasound: Initial imaging modality of choice. Cyst appears anechoic and well-circumscribed. Most are unilocular with thin walls. In the case of prior infection or hemorrhage, may appear heterogenous with internal echoes. CT: Appear as smooth, well-circumscribed cysts at midline near the hyoid bone. They have thin walls and are usually unilocular, although occasionally have septations. They have homogenous fluid or mucoid attenuation of 10-25 HU. MRI: Homogenous low signal on T1. Homogenous high signal on T2 because of fluid content of cyst. Treatment Preoperative ultrasound is perfomed to demonstrate normal thyroid tissue. The thyroglossal duct remnant as well as the central portion of the hyoid bone and cuff of tissue around the tract from the hyoid to the foramen cecum are removed with the Sistrunk procedure to reduce likelihood of recurrence. Discussion
Radiological Presentations Thyroglossal duct cyst on ultrasound. Ahuja et al. Clinical Radiology 2005; 60:141-148.
Ectopic Thyroid Ectopic thyroid results from failure of thyroid tissue to completely descend into the inferior neck. 90% are found at the base of the tongue, but can also occur anywhere along the thyroglossal duct. Ectopic thyroid in the presence of suspected thyroglossal duct cyst is about 1-2%. Before surgery to remove the mass, preoperative ultrasonography should be performed to show normal thyroid with homogenous echogenicity to rule out ectopic thyroid. Patients at high risk (hypothyroid, abnormal TFTs) can have thyroid scintigraphy to confirm thyroid location before surgery. Discussion
Dermoid Cyst Manifest in the 2nd to 3rd decade of life 7% occur in the head and neck with the most common location in the neck being at the base of the tongue. Appear as mobile, midline, slow growing mass In contrast to thyroglossal duct cysts, they are not in close association with the hyoid bone. Can range in size from a few mm to 12 cm Lined with squamous epithelium and can contain sebaceous glands, hair follicles, and sweat glands Discussion
Imaging US: well-circumscribed mass with multiple echogenic foci CT: Appears as thin walled, unilocular mass which is filled with a homogenous, hypoattenuating fluid. Can have characteristic “sack of marbles” appearance due to fat within the fluid. Can also see fluid-fluid levels. May also appear heterogenous due to epithelial secretions. MRI: Variable signal intensity on T1. Usually hyperintense on T2 with clearly demarcated rim and heterogenous internal appearance Discussion
Dermoid cyst. Koeller K K et al. Radiographics 1999;19:121-146.
Branchial Cleft Cyst 95% of branchial cleft anomalies come from the 2nd branchial cleft, 75% of which are cysts. The most common location is anterior to the SCM and lateral to the carotids. They clinically present as painless masses on the lateral neck that enlarge slowly over time. Imaging US: appears as sharply marginated, round to ovoid, centrally anechoic mass with thin wall CT: well-circumscribed, homogenous, hypoattenuated with thin wall MRI: fluid varies from hypointense to slightly hyperintense compared to muscle on T1, hyperintense on T2 Discussion
Cystic Hygroma Most common form of lymphangioma Arises from embryonic lymphatic channels 80% involve the head and neck. In children, most common location is posterior cervical space. In adults, it is seen in sublingual, submandibular, and parotid spaces. They can cross fascial planes because they are very infiltrative. Clinically, often present asymptomatically with painless mass in neck. They are variable in size and can become greater than 10 cm, compressing the airway. Cysts usually contain chylous fluid. Discussion
Imaging US: Appears as multilocular, predominately cystic mass with septae. It also has echogenic areas due to small lymphatics. CT: Appears as a poorly circumscribed, multiloculated mass. It is typically hypoattenuating and may have fluid-fluid levels. MRI: Appears as low intensity on T1. Hyperintense on T2. Discussion Cystic hygroma. Koeller K K et al. Radiographics 1999;19:121-146
Thymic Cyst The thymus and parathyroids arise from the 3rd and 4th pharyngeal pouches. The thymus then descends into the mediastinum through the thymopharyngeal duct, lateral to the thyroid. These can be found anywhere along the thymopharyngeal duct, and usually occur in the first decade of life. Clinically present as slow growing, painless mass on lateral neck. They can present from 1 cm-26 cm. Lined by squamous epithelium with thymic tissue in the cyst wall. Imaging US: unilocular cystic mass extending downward parallel to SCM CT: unilocular or multilocular, hypoattenuating, adjacent to carotid space MRI: hypointense on T1, hyperintense on T2 Discussion
Thyroglossal duct cyst Diagnosis
Ahuja AT, Wong KT, King AD, et al. Imaging for thyroglossal duct cyst: the bare essentials. Clinical Radiology 2005;60:141-148. Brewis C, Mahadevan M, Bailey CM, et al. Investigation and treatment of thyroglossal cysts in children. J R Soc Med 2000;93:18-21.Koch B. Cystic malformations of the neck in children. Pediatr Radiol 2005;35:463–477. Koeller K, Alamo L, Adair C, et al. Congenital cystic masses of the neck: radiologic-pathologic correlation. Radiographics 1999 Jan-Feb;19(1):121-46.Gupta P, Maddalozzo J. Preoperative sonography in presumed thyroglossal duct cysts. Arch Otolaryngol Head Neck Surg 2001;127:200-202.Lim-Dunham J, Feinstein K, Yousefzadeh D et al. Sonographic demonstration of a normal thyroid gland excludes ectopic thyroid in patients with thyroglossal duct cyst. AJR Am J Roentgenol 1995 June;164(6):1489-91. References














![Case Report # []](https://cdn3.slideserve.com/6989602/slide1-dt.jpg)