Download
1 / 47
470 likes | 580 Views
This chapter explores the respiratory system's anatomy and function in supplying oxygen and eliminating carbon dioxide. It details key organs including the nose, pharynx, larynx, trachea, bronchi, and alveoli. The importance of the nasal cavity, pharynx as a passageway, and the larynx's role in routing air and food is emphasized. Additionally, it discusses the structure of bronchi and lungs, pleural membranes, and the mechanics of breathing. Understanding these components is essential for appreciating how oxygen is delivered to cells and carbon dioxide is expelled from the body.

E N D
Chapter 13 The Respiratory System Biology 110 Tri-County Technical College Pendleton, SC
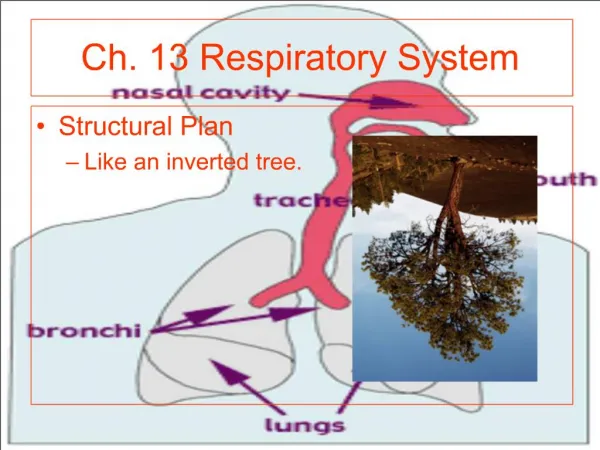
System Essentials • Supply cells with oxygen • Pick up carbon dioxide from the body • Eliminate carbon dioxide from the body • Organs of respiratory system include: Nose, pharynx, larynx, trachea, bronchi and its branches, and the alveoli of the lungs
A nose for this…or that • Only externally visible part of system • Air enters nose through external nares (nostrils) • Interior consists of nasal cavity divided by midline nasal septum • Olfactory receptors in mucosa in superior part of cavity just below ethmoid bone
Nose, cont. • Rest of mucosa lining called respiratory mucosa rests on network of thin-walled veins that warms air flowing past • Mucosa moistens inhaled air & traps incoming debris • Ciliated cells move contaminated mucus posteriorly toward throat (pharynx) swallowed & digested by stomach acid
Nose, cont. • Three mucosa-covered lobes called nasal conchae increase surface area exposed to air • Also increase turbulence in nasal cavity • Nasal cavity separated from oral cavity by partition called the palate • Anterior palate supported by hard bone = hard palate • Posterior palate is unsupported by bone = soft palate
Paranasal Sinuses • Nasal cavity surrounded by paranasal sinuses located in frontal, sphenoid, ethmoid, and maxillary bones • Lighten the skull • Resonance chambers for speech • Produce mucus that drains into nasal cavity • Nasal mucosa continuous throughout RT • Nasal infections can spread throughout mucosa • Sinusitis difficult to treat & can cause marked change in voice quality
Pharynx • Muscular passageway for food and air commonly called throat • Naso-; Oro-; and laryngopharynx • Air enters superior portion (naso) from nasal cavity anteriorly • Air descends through oropharynx and laryngopharynx to enter larynx below • Food from mouth travels with air through oro- and laryngopharynx but directed posteriorly to esophagus instead of entering larynx
Pharynx, cont. • Auditory tubes that drain middle ear open into nasopharynx • otitis media (ear infection) may follow sore throat/pharyngeal infections • Clusters of lymphatic tissue called tonsils found in pharynx • Pharyngeal: (adenoids) located high in naso • Palatine: oropharynx at end of soft palate • Lingual: at base of tongue
Larynx and Associated Structures • Larynx (voicebox) routes air/food into proper channels and plays role in speech • Formed by 8 rigid hyaline cartilages and elastic cartilage called epiglottis • Largest of hyaline cartilages is THYROID cartilage (Adam’s apple) • Epiglottis protects superior opening of larynx
Larynx, cont. • Not swallowing, epiglottis does not restrict passage of air into respiratory passages • Swallowing, larynx pulls forward and epiglottis tips forming lid over opening of larynx • Routes food/drink into esophagus posteriorly • Cough reflexunconscious person
Larynx, cont. • Part of mucous membrane of larynx forms pair of folds called vocal folds (true vocal cords) which vibrate with expelled air • Allows speech • Slitlike passages between folds called glottis • Larynx leads to trachea (windpipe)
Trachea • Extends from larynx to level of 5th thoracic vertebra (~ midchest) • Lined with ciliated mucosa • Walls reinforced with C-shaped rings of hyaline cartilage • Open parts of rings abut esophagus and allow it to expand anteriorly when one swallows
Trachea, cont. • Solid portions support walls and keep it patent (or open) in spite of pressure changes during breathing • Tracheal obstructions are LIFE-threatening • Heimlich maneuver can unclog trachea • It works or my side would be gone…for good • Sometimes emergency trachesostomy is required
Bronchi Divisions • Trachea divides into right and left primary bronchi • Each primary bronchi plunges into medial depression (the hilus-depressed area where vessels enter/leave an organ) of lung • Right pulmonary bronchus is wider, shorter, and straighter than left • Smaller subdivisons of primary bronchi within lung deliver air to alveoli
Lungs and more… • Occupy most of thoracic cavity except for mediastinum (houses heart, great blood vessels, bronchi, esophagus, thymus, and trachea) • Narrow superior portion is APEX; located just deep to clavicle • Broad area resting on diaphragm is BASE • Each lung divided into LOBES by fissures • Left lung = 2 lobes; right lung = 3 lobes
Lungs, cont. • Surface covered by visceral (pulmonary) pleura and walls of thoracic cavity lined by parietal pleura • Membranes produce pleural fluid which allows lungs to glide easily over thorax wall during breathing • Also causes 2 pleural layers to cling together • Glide easily but resist being pulling apart • Absolutely essential for normal breathing
Lungs, cont. • PLEURISY (inflammation of pleura) can be caused by decreased secretion of pleural fluid • Surfaces become dry and roughfriction and stabbing pain with each breath • Another kind of pleurisy results in excess fluid and pressure on the lungs • Primary bronchisecondary & tertiary bronchibronchiolesterminal bronchioles (conducing zone structures)respiratory zone structures
Lungs, cont. • RZ structures include respiratory bronchiolesalveolar ductsalveolar sacsalveoli and is ONLY site of gas exchange
Exchange of Gases • Alveoli composed largely of single layer of layer of squamous epithelial cells • External surface of alveoli covered with cobweb of pulmonary capillaries • Alveolar and capillary walls construct respiratory membrane (air-blood barrier) • Blood flowing on one side; air on the other • Gases diffuse across air-blood barrier by simple diffusion
Gas Exchange, cont. • Surface area of lungs = size of racquetball court (70-80 sq. meters) • Macrophages (dust cells) wander in and out of alveoli to pick up bacteria/debris • Cuboidal epithelial cells scattered throughout alveolar walls secrete surfactant (lipid that coats gas-exchange alveolar surfaces and is important in lung function
Events of Respiration • Pulmonary ventilation (breathing) • External respiration (gas exchange between pulmonary blood and alveoli) • Respiratory gas transport (gas must be transported to/from lungs and tissue cells via bloodstream • Internal respiration (gas exchange between blood and tissue cells at systemic capillaries
Mechanics of Breathing • Pulmonary ventilation depends on volume changes in thoracic cavity • Volume changes lead to pressure changes flow of gases to equalize the pressure • Gas always fills its container • Volume of container related to pressure of gas • Inspiration = gas flowing into lungs • Expiration = gas flowing out of lungs
Mechanics of Inspiration • Diaphragm & external intercostal muscles contract • Size of thorax increaseslungs adhere tightly to thorax wallsstretched to new, larger size of thorax • Lung volume increases producing partial vacuum (pressure less than atmospheric pressure) • Air rushes in to fill space—inspiration is always an active process
Mechanics of Expiration • Usually passive process that essentially reverse of inspiration • Active expiration (forced)—internal intercostals activated and contracted to depress rib cage and abdominal muscles contract to help FORCE air from lungs • Asthma (spasms of bronchioles) or chronic bronchitis/pneumonia can narrow respiratory passageways
Mechanics, cont. • Actelectasis (lung collapse) renders lung useless for ventilation • air enters pleural space through chest wound or rupture of visceral pleural (allows air to enter pleural space from respiratory tract) • Pneumothorax is term given presence of air in intrapleural space (disrupts fluid bond between pleura)
Mechanics, cont. • RESPIRATORY SOUNDS: • Bronchial sounds produced by air rushing through large respiratory passageways such as trachea and bronchi • Vesicular breathing sounds occur as air fills alveoli • Soft and resemble muffled breeze
Modified Respiratory Movements • Situations other than breathing move air in and out of respiratory system • Most “nonrespiratory air movements” are result of reflex activity • Cough, sneeze, crying, laughing, hiccups, yawn, sighing….
External Respiration • Actual exchange of gases between alveoli and blood (pulmonary gas exchange) • Oxygen leaves alveolus and enters blood capillary • Carbon dioxide leaves blood capillary and enters alveolus • Occurs by simple diffusion (movement occurs toward area of lower [ ] of diffusing substance)
Gas Transport • Very small amount of O2 dissolved in blood • Most transported as oxyhemoglobin • Hb + O2 HbO2 • Most CO2 transported as bicarbonate ion • 20-30% carried inside RBCs bound to hemoglobin (at different site than oxygen) • Very small amount transported in plasma • CO2 + H2OH2CO3H+ + HCO3- • For carbon dioxide to diffuse out of blood into alveoli, reaction must be reversed
Internal Respiration • Gas exchange process that occurs between systemic capillaries and tissue cells • Carbon dioxide leaves tissues and enters blood • Oxygen leaves blood and enters tissues • All gas exchanges made according to the laws of diffusion
Respiration Controls • Activity of respiratory muscles, diaphragm, and external intercostals regulated by brain impulses carried by phrenic and intercostal nerves • Respiratory rhythm and depth control center located in medulla and pons • Medulla contains self-exciting inspiratory and expiratory centers • Sets the rhythm of breathing
Controls, cont. • Pons contains apneustic and pneumotaxic centers • Smooth out basic rhythms of inspiration and expiration • Work to maintain ~ 12-15 respirations/min. • EUPNEA= normal breathing rate • Inspiratory center active = inspire • Expiratory center active = expire • Apneustic center in pons=keeps inspiratory center going • Pneumontaxic center in pons=limits length of inspiration and promotes expiration
Rate/Depth Breathing Factors • PHYSICAL such as walking, coughing, and exercise • >body temp can > rate of breathing • CONSCIOUS such as singing, swallowing, or holding breath while swimming • voluntary control limited then involuntary takes over • EMOTIONAL such as fright, surprise, or “other”
Factors, cont. • CHEMICAL most important rate and depth factors • CO2 and O2 levels in blood • Increased levels of CO2 and decreased blood pH MOST important stimuli leading to increase in rate/depth of breathing • Changes in CO2 [ ] in blood act directly on medulla centers • Changes in O2 [ ] in blood detected by chemoreceptors in AORTIC ARCH and CAROTID body in carotid artery
Factors, cont. • Chemoreceptors send impulses to medulla when blood O2 levels are dropping • <s in O2 levels ONLY important when they are dangerously LOW • Increases rate/depth of breathing • Hypoventilation=accumulation of CO2 in blood and >ed blood acidity • Hyperventilation=CO2 removed from blood and <ed blood acidity • Acidosis or alkalosis can result
Respiratory Related Terms • Apena is cessation of breathing caused by hyperventilation • Dyspnea is labored or difficult breathing • Emphysema=alveoli enlarge as walls of adjacent chambers break through; chronic inflammation promotes fibrosis of lungs • Requires lots of energy to exhale • Chronic bronchitis=mucosa of lower respiratory passages become severely inflamed and produces extra mucus
Terms, cont. • Chronic bronchitis impairs ventilation and gas exchange and increases risk of lung infections • Pneumonitis=inflammation of alveoli of the lungs resulting in them becoming clogged with mucus and/or fluids
Volumes and Capacities • Tidal volume (TV) is amount of air moved in and out of lungs with each breath (500 ml) • Inspiratory Reserve Volume (IRV) is amount of air that can be forcibly taken in over tidal volume (2100-3200 ml) • Expiratory Reserve Volume (ERV) is amount of air that can be forcibly exhaled after tidal expiration (1200 ml)
Volumes, cont. • Residual Volume (RV) is amount of air left in lungs that cannot be voluntarily expelled • Vital Capacity (VC) is sum of TV + IRV + ERV • Total amount of exchangeable air • about 4800 ml in healthy young males • Dead space volume is air that remains in conducting zone