Download
1 / 151
1.57k likes | 1.88k Views
SPINAL CORD INJURIES. M.R.EHSAEI M.D ASSOCIATE PROFESSOR OF NEUROSURGERY. Anatomy of spine. Complete spine contains 7 cervical 12 thoracic 5 lumbar 5 sacral 4 coccygeal Spinal cord protection Ligaments. Ligaments of spine. Vertebra (29) 7 cervical, 12 thoracic,

E N D
SPINAL CORD INJURIES M.R.EHSAEI M.D ASSOCIATE PROFESSOR OF NEUROSURGERY
Anatomy of spine • Complete spine contains • 7 cervical • 12 thoracic • 5 lumbar • 5 sacral • 4 coccygeal • Spinal cord protection • Ligaments
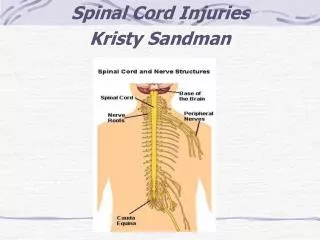
Vertebra (29) 7 cervical, 12 thoracic, 5 lumbar, 5 sacral Conus medullaris at L1-2 vertebrae 31 spinal cord segments 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal C1 dorsal roots missing in some
Cerebrospinal fluid Clear 50-200 mm H2O pressure 0-10 WBC 0 RBC < 45 mg/100 ml protein glucose 2/3 blood level 50-80 mg/100 ml Spinal tap done at L3-L4 Dural sac ends at vert. S1-S2
Cervical Spine • C1 – Atlas • C2 – Axis • Vertebral canal – space for spinal cord • Intervertebral foramen – nerves exit from canal
Anatomy of spine • Anterior column • Half of Vertebral bodies and intervertebral disc • Anterior longitudinal ligament • Middle column • Half of Vertebral bodies and intervertebral disc • posterior longitudinal ligament • Posterior column • Pedicles, facet joints, lamina • Supraspnious, interspinous, infraspinous ligaments
SPINAL CORD INJURIES Car Crashes: 83% Motorcycle incidents: 10% Bicycle accidents: 3% Medical/Surgical Complications: 38% Hit by falling Object: 30% Pedestrian: 22% Gunshot: 92% Personal Contact: 6% Diving: 55% Snow skiing: 8% Surfing: 6% Source: National Spinal Cord Injury Statistical Center
Epidemiology • Spinal injury • Motor vehicle crashes :41% • Falling down :21% • Sporting activity:8% • Human violence:22% • Others:8% • Average age : 34yrs • M:F = 4:1
Epidemiology • Approx. 100,000 new cases/year, 80% male. Age group most commonly injured: 16-30 years (43%) and 31-45 (28%). • Although Vehicle is the leading cause overall, Falls become the leading cause in people over 60 years.
Spinal Cord Injuries • Traumatic injury of vertebral and neural tissues due to compressing, pulling or shearing forces • Most common locations: cervical (1&2), cervical (4-7), and 12th thoracic – 2nd lumbar vertebrae • Locations reflect most mobile portions of vertebral column and the locations where the spinal cord occupies most the the vertebral canal
Spinal Cord Injuries • Vertebral injury can occur due to fracture, dislocation, or both. • Within minutes after injury, hemorrhages appear in the central gray matter, pia, and arachnoid. • Local hemorrhages reduce vascular perfusion
General Symptoms & Signs : • Pain &Tenderness • Skin abrasions or contusions • Subcutaneous Hematoma • Muscle Spasm • Cripitation in Touch • SpinalDeformity
Neurological Exam: • Detection & Documentation : • Sensory Level • Posterior Column function • Sacral Sensory Sparing • Muscle Weakness (0 - 5 ) • Pathological Reflex (BCR & Babinski) • Rectal Exam for Tone & cotracture
Neurological evaluation: • Complete inj.:no motor or sensory function below the zone of inj. • Incomplete inj.:partial preservation of motor or sensory function below the zone of inj.
Neurological evaluation:cervical inj. • Incomplete inj.: • Ant cord syn. • Central cord syn. • Brown-sequard syn. • Post.cord syn. • Spinal shock: • hypotension without tachycardia (motor,sensory,and reflexes are absent but cannot determine complete inj.until bulbocavernosus or other reflexes return within 24 houres.)
Incomplete Spinal Cord Lesions • The anterior cord syndrome • cervical flexion injuries causing cord contusion • protrusion of a bony fragment or herniated intervertebral disk into the spinal canal • laceration or thrombosis of the anterior spinal artery • rarely, systemic embolization or prolonged cross-clamping of the aorta during resuscitation or surgery
Incomplete Spinal Cord Lesions • central cord syndrome (m/c) • affects the central gray matter and the most central portions of the pyramidal and spinothalamic tracts • a greater neurologic deficit in the upper extremities than in the lower extremities
Incomplete Spinal Cord Lesions • The Brown-Séquard syndrome, or hemisection of the spinal cord • a penetrating lesion such as a gunshot or knife wound • ipsilateral motor paralysis and contralateral sensory hypesthesia distal to the level of injury
Neurologic status : frankel scale • a) no motor or sensory function • b) sensation but no motor function • c) motor function present but useless • d) motor function present but useful • e) normal motor and sensory
Neurologic exam: cervical inj. • C4(spont.breathing),C5(deltoids and biceps) C6(wrist ext.),C7(triceps and wrist ext.),C8 (finger flex.),T1(intrinsics). • Sensory:C5(upper outer arm),C6(thumb),C7 (long finger),C8(little finger),T1(medial forearm).
Prognosis of spinal cord inj.: • Complete inj: usually remains complete,but one or two level recovery is expected. • Incomplete inj.:have potential for significan t recovery, particlarly in bronwn-sequard and central cord syn.
Prognosis of spinal cord inj.: • Gunshot wound to the spine with spinal cord inj.carry a poor prognosis for recovery. • Spinal cord recovery is better if bony impingment is removed for incomplete type. • Patients with congenital C1-C2 instability and congenital stenosis have higher incidence of spinal cord inj.
Prognosis of spinal cord inj.: • Patient with ankylosing spondylitis often sustain unstable three-column inj.,even with minor trauma. • High dose corticosteroid is administrated early to patient within 8 hours of inj. to improve the prognosis.
RADIOLOGICAL studies: • Plain x-ray: Ap--LAT--Open mouth—Oblique- Pillar view--Stretch test--Flexion/Extension view • Tomography • C.T scan :best modality for bony lesion. • Myelography • C.T myelography • M.R.I: best for soft tissue and give prognosis after inj.
Upper cervical inj. • occipital condylar fx. • occiput-c1 dislocation. • C1-C2 subluxation. • fracture of C1. • frature of odontoid. • fracture through the pedicle of C2.
Occipital condylar fx. • diagnosis with tomogram or C.T scan. • lig.inj, I.c.hematoma,and neurological deficit may accompany this inj. • treatment: • usually rigid orthosis or halo vest for 3 m. • flex/ext film is obtained at 3 m. • occiput to c2 fusion if resultant instability.
occiput-c1 dislocation: # flex/ext force on the head. #disruption of all lig. #unstable and always fatal. #treatment:occiput-c1 fusion.
C1-C2 subluxation: • Rupture of transverse lig. • Atlantodens interval: • 3-5mm indicate rupture of transverse lig. • >7-8mm indicate all lig.disruption. • >10mm causes spinal cord compression. • Treatment: • if instability 3-5mm==>halo for 2-3 m then dynamic study repeated.if instability >4mm then needs fusion c1-c2. • if instability >5mm then early fusion c1-c2.
C1-C2 subluxation: • Atlantoaxial rotatory fixation: the head is tilted toward the side of fixation and the chin and c2 spinous process is pointed toward the opposite direction. • Type 1: rotatory fixation with no ant. displacement. • Type 2: rotatory fixation with 3-5mmant.displacem. • type3: rotatory fixation with>5mm ant displacement • Type4:rotatory fixation with post.displacement. • tratment: reduction&c1-c2 fusion if unstable.
Stable Upper cervical Injuries: • Atlas fractures: • ant. arch fx. • post. arch fx. • lat. mass fx.with less displacement. • Axis fractures: • type 1 odontoid fx. • hangman fx.without angulation.
Fracture of C1: • Axial loading usually with breaks at two sites. • >7mm widening of lat.mass==>trnsverse lig.rupture .==>first immobilization with hallo for 2-3m and C1-C2 fusion may be performed if instability is greater than 5mm.
Fractures of odontoid: • Type 1:rare,avulsion fracture of the tip. stable and treatment is cervical collar. • type 2: fracture at the base of the odontoid. • ant .displ.(flex.inj.) is more common than post displ.(ext.inj.). • nonunion rate is 20-80% especially age >50 y. • Type 3:fracture through the body. • nondisplaced: cervical orthosis or halo. • displaced: halo jacked for 3m.
ODONTOID FX FIXATION OF ODONTOID
Fractures through pedicle of C2: • Mechanism of Hangman fracture :ext.inj. • Types: • type 1: minimal displacement(less than 3mm) • type 2: significant displacement (>3mm) and angulation(>11 deg.) • type 2A: minimal displacement(<3mm) and angulation(>11 deg.) • type 3: associated facet dislocation.
Fractures through pedicle of C2: • Treatment: • type 1: halo jacket for 12 w. • type 2:traction for 2-3w for reduction +halo for 10-12w. • type 2A: no traction,extention,and compression,halo for 3m. • type 3 or late instability or nonunion: ant.C2-C3 fusion or post pedicular screw fixation(C2-C3 plating.
M.R.I of cervical At C4-C5 , Disruption and Widening of the intervertebral Disc, compression fracture of C5, anterolisthesis of C4-C5
Facet fracture/dislocation: • UNILATERAL OR BILATERAL. • MAY BE WITH DISC HER. & CORD COMP. • IN UNILATERAL :DISPLACEMENT IS ABOUT 25% • IN BILATERAL :DISPLACEMENT IS ABOUT 50 %.