Download
1 / 45
460 likes | 638 Views
DIZZINESS. History. Spinning History of 1 st episode Predisposing factors Associated symptoms How long? Single or recurrent. Homework. Chondrodermatitis nodularis chronica helicis Hallpike test Epley’s manouver. The Nose. Anatomy. Anatomy. # nasal bones. Epistaxis.

E N D
DIZZINESS History • Spinning • History of 1st episode • Predisposing factors • Associated symptoms • How long? • Single or recurrent
Homework • Chondrodermatitisnodularischronicahelicis • Hallpike test • Epley’smanouver
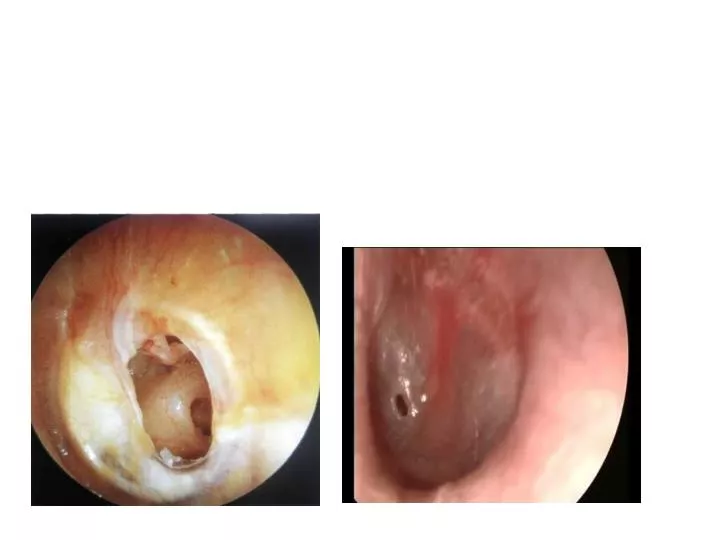
Septal perforation • Trauma ,iatrogenig,Wegner’s ,sarcoidosis,TB,Syphilis, COCAINE,NEOPLASTIC. • Asynptomatic, wistling,blockage,epistaxis • FBC,ESR,CANCA,ACE level?VDRL.Biopsy • Saline nasal douches ,surgical
Rhinitis • 2 out of 3 for >1 hour every day for >2 weeks. -Nasal congestion -rhinorrhoea (Ant. Or Post.) -sneezing - itching (nasal cavity),facial pain ,anosmia *RAST *steroides (beclomethazone,fluticasone,mometasone) *Antihistaminics *Oral steroides *Montelukast *saline douches *surgical NB Rhinits and sinusits usually coexist and are concurrent in most individuals; thus, the correct terminology is now rhinosinusits.
Sinusitis • Acute:<4 weeks 1-Broad spectrum antibiotics 2-Betnesol nasal drops(2 drops BD) 3-Steam inhalation 4-Xylometazoline 0.5% 2 drops tds • Chronic >12 weeks RAST ,ESR,CANCA,ACE,CT scan Sinuses Medical treatment for 3 months mild :fluticasone 2 puffs OD Severe (polyps) :Betamethasone 2 drops for 6 weeks followed by steroides spray Oral antihistaminics (if allergic) Oral steroids (very severe) Oral antibiotics (clarythromycin) Surgical: FESS Referral: failure of treatment red flags patient willing to have surgery.
Nasal polyps Around in 1% of adults in the UK have nasal polyps. They are around 2-4 times more common in men and are not commonly seen in children or the elderly. • What are they? • Paediatric polyps? • ?Unilateral polyps?( neoplastic until proven otherwise) • Associated with Asthma (particularly late-onset asthma) Aspirin sensitivity..........Samter's triad infective sinusitis cystic fibrosis Kartagener's syndrome Churg-Strauss syndrome • all patients with suspected nasal polyps should be referred to ENT for a full examination • topical corticosteroids shrink polyp size in around 80% of patients
Red flags Unilateral blockage Unilateral discharge Blood stained discharge Eye signs /symptoms Facial swelling (smokers, elderly)
SNORING • Causes • Epworth sore...?sleep apnoea(is it witnessed) • Day time somnolesence • Treatment Wight loss Surgical UVPPP CPAP • DLVA Patient’s responsibility to inform DVLA when OSA suspected/investigated. Doctors responsibility to inform DVLA if untreated OSA pt is witnessed driving
Homework • CSF rhinorrhoea
Acute tonsillitis Acute tonsillitis
NICE indications for antibiotics • features of marked systemic upset secondary to the acute sore throat • unilateral peritonsillitis • a history of rheumatic fever • an increased risk from acute infection (such as a child with diabetes mellitus or immunodeficiency) • patients with acute sore throat/acute pharyngitis/acute tonsillitis when 3 or more Centorcriteria are present • WHICH ANTIBIOTICS? Presence of tonsillarexudate Tender anterior cervical lymphadenopathy or lymphadenitis History of fever Absence of cough
Hoarseness • Causes: URTI (Most common) Trauma(shouting/nodules). Iatrogenic tumour neurological (?) functional(young women) Ask about ? Reflux symptoms , Wight loss, inhalers use, voice misuse, stress ,swallowing, breathing • Investigations :TFT,weight ,indirect laryngoscopoy. • Urgent Chest XRAY (IF SYMPTOMS >3 WEEKS) • If X-ray shows positive signs ..urgent referral to chest physician • If X-ray shows negative signs ..urgent referral to ENT • Early laryngeal tumours confined to vocal cords have 80-90% 5 Y survival .
2WW Red flags Persistent hoarseness > 3 weeks Pain Dysphagia Haemoptysis Otalgia Neck lump Especially in - smokers - over 40yrs
Neck lumps • Lymphadenopathy • Branchial cyst • Thyroglossal cyst • Salivary glands • Refer urgently to ENT
Urgent referral • Mouth ulcers> 3weeks. • Lumps in mouth >3 weeks • Ubexplained sore throat>1 month • Hoarseness >3 weeks, negative CXR. • Unexplained salivary gland swelling>4 weeks • Unilateral unexplained ear ache with normal otoscopy • Asymmetrical /unilateral deafness • Unilateral tinnitus
The ear http://www.youtube.com/watch?feature=player_embedded&v=0kEKoQ33dB0