Download
1 / 28
300 likes | 637 Views
Cardiovascular Risk Factor Overview and Management. Nathan D. Wong , PhD, FACC Associate Professor and Director, Heart Disease Prevention Program, University of California, Irvine.

E N D
Cardiovascular Risk Factor Overview and Management Nathan D. Wong, PhD, FACC Associate Professor and Director, Heart Disease Prevention Program, University of California, Irvine
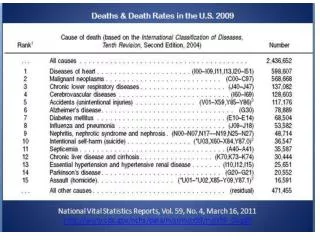
Cardiovascular Disease: The Leading Cause of Death in US Women in 1995 Heart disease 375 Cerebrovascular disease 96.4 Lung cancer 60.6 COPD* 48.9 Pneumonia/Influenza 45.1 Breast cancer 43.8 Accidents 31.9 Diabetes 33.1 Ovarian cancer 9.9 0 50 100 150 200 250 300 350 400 Deaths (1,000) *COPD=chronic obstructive pulmonary disease. Adapted from Anderson RN et al. Monthly Vital Statistics Report.Vol 45(suppl 2):June 12, 1997.
CHD is the single largest killer of men and women ~13.9 million have history of MI and/or angina Each year 1.1 million people have MI 370,000 die of MI, 250,000 die within 1 hr By age 60, every 5th man and 17th woman develops CHD 1998 estimated direct and indirect costs of heart disease are $95.6 billion 53.3 million adults have elevated LDL-C and warrant intervention (1994 NHANES data) 22.3 million qualify for drug therapy, 5.5 million receive therapy CHD in the United States AHA. 1998 Heart and Stroke Statistical Update; 1997. National Center for Health Statistics. National Health and Nutrition Examination Survey (III);1994. (Data collected 1991-1994.)
CVD Mortality Trends for Males and Females* 520 500 480 Deaths inthousands 460 440 420 20 0 87 89 91 93 95 1979 81 83 85 1996 Years Males Females *United States: 1979-1996 mortality. AHA. 1999 Heart and Stroke Statistical Update; 1998.
30 20 10 0 15-19 20-24 25-29 30-34 PDAY: Percentage of Right Coronary Artery Intimal Surface Affected With Early Atherosclerosis Raised lesions 30 30 Women Men Fatty streaks 20 20 10 10 0 0 Intimalsurface(%) 15-19 20-24 25-29 30-34 15-19 20-24 25-29 30-34 White White 30 20 10 0 15-19 20-24 25-29 30-34 Black Black Age (y) PDAY=Pathobiological Determinants of Atherosclerosis in Youth. Strong JP, et al. JAMA. 1999;281:727-735.
LipidsHTNDiabetes Behavioral HemostaticThrombotic Inflammatory Genetic Beyond Cholesterol: Predicting Cardiovascular Risk In the 21st Century Cardiovascular Risk
Continuum of Patients at Risk for a CHD Event Post MI/Angina Secondary Prevention Other Atherosclerotic Manifestations Subclinical Atherosclerosis PrimaryPrevention Multiple Risk Factors Low Risk Courtesy of CD Furberg.
Total Cholesterol Distribution: CHD vs Non-CHD Population Framingham Heart Study—26-Year Follow-up No CHD 35% of CHD Occurs in People with TC<200 mg/dL CHD 150 300 250 200 Total Cholesterol (mg/dL) Castelli WP. Atherosclerosis. 1996;124(suppl):S1-S9. 1996 Reprinted with permission from Elsevier Science.
Low HDL-C Levels Increase CHD Risk Even When Total-C Is Normal (Framingham) 12.50 11.91 11.91 14 9.05 10.7 11.24 12 6.6 10 5.53 3.83 6.56 8 14-y incidence rates (%) for CHD 4.85 6 4.67 260 2.06 4.15 3.77 4 2.78 230–259 2 200–229 Total-C (mg/dL) 0 < 200 < 40 40–49 50–59 60 HDL-C (mg/dL) Risk of CHD by HDL-C and Total-C levels; aged 48–83 y Castelli WP et al. JAMA 1986;256:2835–2838
CHD Incidence Related to HDL-C Levels in Various Trials CHD incidence Women Men 0 -2 % change in risk per 1 mg/dL increment in HDL-C -4 -6 -8 -10 LRCF FHS CPPT FHS LRCF MRFIT 95% confidence intervals (CIs) for adjusted proportional hazards regression coefficients. Gordon DJ et al. Circulation 1989;79:8–15
Clinical Benefits of Cholesterol Reduction • A recent meta-analysis of 38 trials demonstrated that for every 10% reduction in TC • CHD mortality decreased by 15% (P<0.001) • total mortality decreased by 11% (P<0.001) • Decreases were similar for all treatment modalities • Cholesterol reduction did not increase non-CHD mortality Gould AL et al. Circulation. 1998;97:946-952.
Positive risk factors Age male ³45 female ³55 Family Hx of CHD: 1st-degree relative with MI or sudden cardiac death - male relative: <age 55 female relative: <age 65 Current cigarette smoking Hypertension: BP ³140/90 mm Hg or on antihypertensive meds Low HDL-C: <40 mg/dL Diabetes IS A CHD QUIVALENT IDENTIFYING PT AS HIGH RISK Negative risk factor High HDL-C: 60 mg/dL Major CHD Risk Factors Other Than LDL-C According to NCEP ATP-III
Other Recognized Risk Factors • Obesity: traditionally determined by body mass index >30 kg/m2 with overweighted defined as 25-<30 kg/m 2. • Abdominal obesity involves waist circumference >40 in. in men, >35 in. in women • Physical inactivity: various definitions
JNC VI: Risk Stratification and Treatment* Group AGroup BGroup C Uncomplicated HTNHTN w/Risk FactorsTOD/ CCD/Diabetes High-normal Lifestyle Lifestyle Drug therapy‡(130-139/85-89) modification modification Stage 1 Lifestyle Lifestyle Drug therapy(140-159/90-99) modification modification† (up to 12 mo) (up to 6 mo) Stages 2 and 3 Drug therapy Drug therapy Drug therapy(160/ 100) JNC VI. November 1997:chapter 2. NIH publication 98-4080.
Probability of Death From CHD in Patients With NIDDM and in Nondiabetic Patients, With and Without Prior MI 100 80 60 Survival (%) 40 Nondiabetic subjects without prior MI Diabetic subjects without prior MI Nondiabetic subjects with prior MI Diabetic subjects with prior MI 20 0 5 6 3 4 7 2 8 0 1 Years Kaplan-Meier estimates Haffner SM et al. N Engl J Med 1998;339:229–234
Definitions of Diabetes and Impaired Fasting Glucose • New ADA definition (1998) defines fasting blood sugar of > 126 mg/dl as diabetes, casual blood glucose > 200 mg/dl. Impaired fasting glucose is 110-125 mg/dl • Diabetic control generally defined as HgbA1c <8%. • BP recommended <130/80 mmHg, LDL-C goal <100 mg/dl
Secondary CHD Prevention in Women: Results from the CARE Trial • CARE was a secondary prevention trial of pravastatin versus placebo treatment in 4159 men and women with average lipid levels over 5 years • 576 post-menopausal women were randomized; average age 61; 10% on HRT • Average baseline lipids: TC 215 mg/dL, LDL-C 140 mg/dL, HDL 45 mg/dL • 5 year treatment results: 46% reduction in all coronary events, 48% reduction in PTCA, 40% reduction in CABG, 56% reduction in stroke JACC 1998;32:140-146
Heart and Estrogen/Progestin Replacement Study (HERS): Secondary Prevention of CHD in Women • Randomized, placebo-controlled trial of E/P therapy vs. placebo in 2763 women with CHD; average age 67 years • Treatment was 0.625 mg CEE + 2.5 mg medroxyprogesterone daily for 4 years • Primary endpoint: nonfatal MI and CHD death • Secondary endpoints: CABG, PTCA, unstable angina, CHF, PVD, TIA JAMA 1998;280:605-613
HERS Results • Non-fatal MI HRT 116 Placebo 129CHD death HRT 71 Placebo 58 • End of Year 1 CHD events (HRT) 42.5/1000 women-years CHD events (Plac) 28/1000 women-years • Year 4-5: CHD events (HRT) 23/1000 women-years CHD events (Plac) 34.3/1000 women-years • DVT/PE HRT 6.3 vs. Plac 2.2 Cholelithiasis HRT 84 vs. Plac 62 JAMA 1998;280:605-613
HERS Results • No statistically significant difference between HRT and placebo in both primary and secondary endpoints after 4 years. • Within first year, greater incidence in CHD events in HRT group. In years 3 and 4, lower CHD events in HRT group compared to placebo. • HRT lowered LDL 11% and increased HDL 10% compared to placebo. • Approximately 50% of randomized women were on lipid-lowering drugs. • Higher incidence of VTE and cholelithiasis in HRT group. JAMA 1998;280:605-613
Is there clinical evidence that inflammatory markers predict future coronary events and provide additional predictive information beyond traditional risk factors?
hs-CRP and Risk of Future MI in Apparently Healthy Men P Trend <0.001 P < 0.001 P < 0.001 P = 0.03 Relative Risk of MI 1<0.055 20.056–0.114 30.115–0.210 4>0.211 Quartile of hs-CRP (range, mg/dL) Ridker PM et al. N Engl J Med 1997;336:973-979.
hs-CRP and Risk of Future Cardiovascular Events in Apparently Healthy Women P Trend <0.002 Any Event MI or Stroke Relative Risk 1<0.15 20.15–0.37 30.37–0.73 4>0.73 Quartile of hs-CRP (range, mg/dL) Ridker PM et al. Circulation 1998;98:731-733.
Lp(a) in Atherogenesis: Another Culprit? • Identical to LDL particle except for addition of apo(a) • Plasma concentration predictive of atherosclerotic disease in many epidemiologic studies, although not all • Accumulates in atherosclerotic plaque • Binds apo B-containing lipoproteins and proteoglycans • Taken up by foam cell precursors • May interfere with thrombolysis Maher VMG et al. JAMA. 1995;274:1771-1774. Stein JH, Rosenson RS. Arch Intern Med. 1997;157:1170-1176.
Lp(a): An Independent CHD Risk Factor in Men of the Framingham Offspring Cohort 10 5 3.6 2.7 2 1.9 1.8 1.8 1.2 1 RR 0.5 Lp(a) TC HDL-C HT GI Smoking 0.2 0.1 RR=relative risk; HT=hypertension; GI=glucose intolerance. Bostom AG et al. JAMA. 1996;276:544-548.
Homocysteine: Role in Atherogenesis • Linked to pathophysiology of arteriosclerosis in 1969 • CVD patients have elevated levels of plasma homocysteine • May cause vascular damage to intimal cells • Elevated levels linked to: • genetic defects • exposure to toxins • diet • Increased dietary intake of folate and vitamin B6 may reduce CVD morbidity and mortality