Download

1 / 11
110 likes | 227 Views
The Integrated Resource Framework (IRF) emphasizes the pivotal role of clinicians and care professionals in resource management, moving beyond traditional financial departments. Successful governance structures must grant clinicians the freedom to act while ensuring accountability. The IRF is influenced by challenges like demographic and economic pressures, necessitating a shift towards integrated health and social care. The Triple Aim framework fosters improved population health, individual experiences, and cost reduction. Engagement of clinicians is crucial to reshape patient pathways and optimize resource distribution for better outcomes.

E N D
The Integrated Resource Framework Dr Sheena MacDonald Senior Medical Advisor
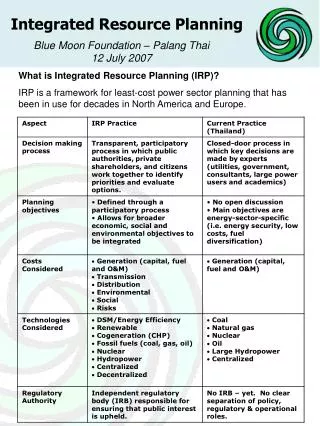
Starting Point for the IRF… It’s not just about Finance Departments “Clinicians & Care Professionals.. have a crucial role... It is they who commit resources.” “Governance structures need to allow them freedom to act and to ensure there is accountability for their actions.”“Finance needs to be structured in a way that supports this.” Prescription for Partnership Audit Commission Dec 2007
Integrated Resource Framework Context - a perfect storm Demographic pressures Economic pressures Planning in the margins of historic activity Marginal or strategic planning? Performance or variation? Bottom line or opportunity cost? Administration or stewardship?
Integrated Resource Framework • Policy • Partnership working across health and social care • Shifting the Balance of Care • NHS Quality Strategy • Reshaping Care for Older People • Two planning disconnects • Within health – between primary/community and acute • Between health and social care • Need to shift resources to support shift towards better, • more appropriate care – and better outcomes
Integrated Resource Framework Triple Aim • IRF underpinned by the Triple Aim of a rational care organisation, defined by the Institute of Health Improvement (IHI) as: • Improving population health • Improving individual experience • Reducing costs • Each test site will use an “integrator” structure to direct resource use across health and social care and oversee progress towards the Triple Aim.
Some supposedly simple questions: Do you know how much you spend per head on people over 75 yrs? Across Health and Social Care? Is there variation: by locality? by GP? in the type of care provided? in outcomes? Integrated Resource Framework
Diagnostics – Endoscopic GP Referrals to all Nationally Reported Endoscopic Tests – April 08 to March 2009 12 10 8 GP Referrals by 500 Patients 6 4 2 0 F A B C H G E D J I T K P V Y N R Q U L S O M W X GP Practice
Emergency Inpatient Admissions Total Emergency Admissions to General Medicine, GP Acute and DME Beds by Practice - 2008/09 40 45 40 35 35 30 30 25 25 20 Distance from the BGH Admissions per 500 of total population 20 15 15 10 10 5 5 0 0 A B E C D J L F T K P S V X Y H N R U G O Q M W I Gp Practice General Medicine BGH Emergency Admissions DME Community & BGH Emergency Admissions GP Acute Community & BGH Emergency Admissions Out of Area Emergency Admissions Mileage
Referrals to A&E GP Referrals to A&E 2005/06 – 2008/09 Chart 17 - GP Referrals to A&E per 500 patients for 2005/06 to 2008/09 90 80 70 60 50 Referrals per 500 Patients 40 30 20 10 0 F A B E C D H G I J L T K P S V X Y Z N R U O Q M W Practice 2005/06 2006/07 2007/08 2008/09
Outpatient Referrals Comparison of Outpatient Referrals to the BGH and Out of Area by Practice for 2008/9 180 45 160 40 140 35 120 30 100 25 Referrals by 500 Practice Population Mileage to BGH 80 20 60 15 40 10 20 5 ` 0 0 I J L F T A B E K P S V C D H N R U G O Q M W X Y GP Practice Borders Other Scottish Other English Mileage
Moving Forward……. • How do we engage clinicians • Where do we, as clinicians, influence the patient pathway and the concomitant distribution of resources • Where and how could we influence the patient pathway if the current constraints imposed upon us by lack of integrated resources were removed