Download
1 / 67
680 likes | 714 Views
Explore surface features, muscle anatomy, and vein classifications of the thigh and lower limb. Learn about varicose veins, venous pump, and operative treatments.

E N D
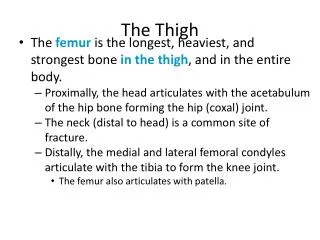
The Thigh I Dr. Fadel Naim Orthopedic Surgeon IUG
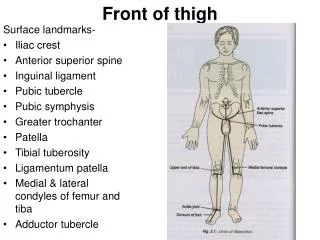
Surface anatomy of the thigh • Surface features of the Thigh • Sartorius muscle • Quadriceps femoris muscle • Adductor longus muscle • Hamstring muscles • Femoral triange
VEINS OF THE LOWER LIMB • The veins of the lower limb can be divided into three groups: • Superficial • Deep • perforating. • The superficial veins • consist of the great and small saphenous veins and their tributaries • situated beneath the skin in the superficial fascia. • The constant position of the great saphenous vein in front of the medial malleolus should be remembered for patients requiring emergency blood transfusion. • The deep veins are • the venae comitantes to the anterior and posterior tibial arteries • the popliteal vein • the femoral veins and their tributaries. • The perforating veins • communicating vessels that run between the superficial and deep veins. • Many of these veins are found particularly in the region of the ankle and the medial side of the lower part of the leg. • They possess valves that are arranged to prevent the flow of blood from the deep to the superficial veins.
Superficial Veins The great saphenous vein • Drains the medial end of the dorsal venous arch of the foot • Passes upward directly in front of the medial malleolus • It then ascends in company with the saphenous nerve in the superficial fascia over the medial side of the leg. • The vein passes behind the knee and curves forward around the medial side of the thigh
Superficial Veins The great saphenous vein • It passes through the lower part of the saphenous opening in the deep fascia and joins the femoral vein about 1.5 in. (4 cm) below and lateral to the pubic tubercle • The great saphenous vein possesses numerous valves • Connected to the small saphenous vein by one or two branches that pass behind the knee. • Several perforating veins connect the great saphenous vein with the deep veins along the medial side of the calf
At the saphenous opening in the deep fascia, the great saphenous vein usually receives three tributaries: • The superficial circumflex iliac vein • the superficial epigastric vein • the superficial external pudendal vein. • These veins correspond with the three branches of the femoral artery found in this region. • An additional vein, known as the accessory vein, usually joins the main vein about the middle of the thigh or higher up at the saphenous opening.
VENOUS PUMP OF THE LOWER LIMB • Venae comitantes are subjected to intermittent pressure at rest and during exercise in the closed fascial compartments of the lower limb. • The pulsations of the adjacent arteries help move the blood up the limb. • The contractions of the large muscles within the compartments during exercise compress these deeply placed veins and force the blood up the limb. • The superficial saphenous veins, are not subject to these compression forces. • The valves in the perforating veins prevent the high-pressure venous blood from being forced outward into the low-pressure superficial veins. • As the muscles within the closed fascial compartments relax,venous blood is sucked from the superficial into the deep veins.
VARICOSE VEINS • A varicosed vein is one that has a larger diameter than normal and is elongated and tortuous. • Commonly occurs in the superficial veins of the lower limb • Responsible for considerable discomfort and pain. • Many causes: • Hereditary • Weakness of the vein walls • Incompetent valves • Elevated intra-abdominal pressure • Thrombophlebitis of the deep veins • By incompetence of a valve in a perforating vein: • High-pressure venous blood escapes from the deep veins into the superficial veins and produces a varicosity • Operative treatment of varicose veins • The ligation and division of all the main tributaries of the great or small saphenous veins, to prevent a collateral venous circulation from developing • It is imperative to ascertain that the deep veins are patent before operative measures are taken.
GREAT SAPHENOUS VEIN CUT DOWN • Usually performed at the ankle • Disadvantage that phlebitis is a potential complication • Also at the groin in the femoral triangle, • Phlebitis is relatively rare • Larger diameter of the vein • Use of large-diameter catheters • Rapid infusion of large volumes of fluids.
The Great Saphenous Vein In Coronary Bypass Surgery • In occlusive coronary disease caused by atherosclerosis, the diseased arterial segment can be bypassed by inserting a graft consisting of a portion of the great saphenous vein. • The venous segment is reversed so that its valves do not obstruct the arterial flow. • Following removal of the great saphenous vein at the donor site, the superficial venous blood ascends the lower limb by passing through perforating veins and entering the deep veins. • The great saphenous vein can also be used to bypass obstructions of the brachial or femoral arteries
Inguinal Lymph Nodes • The inguinal lymph nodes are divided into superficial and deep groups. • Superficial Inguinal Lymph Nodes • lie in the superficial fascia below the inguinal ligament • divided into a horizontal and a vertical group • The horizontal group • lies just below and parallel to the inguinal ligament • The medial members of the group receive superficial lymph vessels from the anterior abdominal wall below the level of the umbilicus and from the perineum • urethra, the external genitalia of both sexes (but not the testes) • the lower half of the anal canal • The lateral members of the group receive superficial lymph vessels from the back below the level of the iliac crests
Superficial Inguinal Lymph Nodes Horizontal Group Vertical Group Dr. Vohra
Inguinal Lymph Nodes • The vertical group • Lies along the terminal part of the great saphenous vein and receives most of the superficial lymph vessels of the lower limb • The efferent lymph vessels from the superficial inguinal nodes pass through the saphenous opening in the deep fascia and join the deep inguinal nodes.
Inguinal Lymph Nodes • Deep inguinal lymph nodes • Located beneath the deep fascia and lie along the medial side of the femoral vein • The efferent vessels from these nodes enter the abdomen by passing through the femoral canal to lymph nodes along the external iliac artery
LYMPHATICS OF THE LOWER LIMB • The superficial and deep inguinal lymph nodes drain: • All the lymph from the lower limb • Drain lymph from the skin and superficial fascia of: • The anterior and posterior abdominal walls below the level of the umbilicus; • Lymph from the external genitalia and the mucous membrane of the lower half of the anal canal • Patient may present with an enlarged, painful inguinal lymph node caused by lymphatic spread of pathogenic organisms that entered the body through a small scratch on the undersurface of the big toe.
SUPERFICIAL FASCIA OF THE THIGH • The membranous layer of the superficial fascia of the anterior abdominal wall extends into the thigh and is attached to the deep fascia (fascia lata) about a fingerbreadth below the inguinal ligament • The fatty layer of the superficial fascia on the anterior abdominal wall extends into the thigh and continues down over the lower limb without interruption
DEEP FASCIA OF THE THIGH (FASCIA LATA) • The deep fascia encloses the thigh like a trouser leg • At its upper end is attached to the pelvis and the inguinal ligament • On its lateral aspect, it is thickened to form the iliotibial tract • The iliotibial tract receives the insertion of • Tensor fasciae latae • Greater part of the gluteus maximus muscle • In the gluteal region, the deep fascia forms sheaths, which enclose • The tensor fasciae latae • The gluteus maximus
Saphenous Opening • The saphenous opening is a gap in the deep fascia in the front of the thigh just below the inguinal ligament. • It transmits: • the great saphenous vein • some small branches of the femoral artery • lymph vessels • The saphenous opening is situated about 1.5 in. (4 cm) below and lateral to the pubic tubercle.
Saphenous Opening • The falciform margin is the lower lateral border of the opening, which lies anterior to the femoral vessels • The border of the opening then curves upward and medially, and then laterally behind the femoral vessels, to be attached to the pectineal line of the superior ramus of the pubis. • The saphenous opening is filled with loose connective tissue called the cribriform fascia.
FASCIAL COMPARTMENTS OF THE THIGH • Three fascial septa pass from the inner aspect of the deep fascial sheath of the thigh to the linea aspera of the femur • the thigh is divided into three compartments, each having muscles, nerves, and arteries. • The compartments are • Anterior • Medial • posterior
Anatomy of the thigh Thigh innervations: Anterior compartment from femoral nerve L2,3,4. Medial compartment from obturator nerve L2,3,4. Posterior compartment from sciatic nerveL4,5,S1,2,3 (sacral plexus).
Thigh innervations Anterior compartment- Extensors of the knee Femoral Nerve femur medial lateral Medial compartment- Adductors of the knee Obturator Nerve Posterior compartment- Flexors of the knee Sciatic Nerve
CONTENTS OF THE ANTERIOR FASCIAL COMPARTMENT OF THE THIGH • Muscles: • Sartorius • Iliacus • Psoas • Pectineus • quadriceps femoris. • Blood supply: • Femoral artery. • Nerve supply: • Femoral nerve.
Sartorius • A narrow, strap-shaped muscle that covers the femoral artery in the middle one third of the thigh. • Origin: • From the anterior superior iliac spine. • Insertion: • The muscle fibers run downward and medially • Attached to the upper part of the medial surface of the shaft of the tibia. • Nerve supply: • Femoral nerve. • Action: • At the hip joint • Flexes • Abducts • Laterally rotates the thigh • At the knee joint • Flexes • Medially rotates the leg.
Iliacus • Origin: • This fan-shaped muscle arises from the iliac fossa within the abdomen • Insertion: • The fibers converge and join the tendon of the psoas to form the iliopsoas muscle • Nerve supply: • A branch of the femoral nerve within the abdomen. • Action: • Flexes the thigh on the trunk at the hip joint • If the thigh is fixed, it flexes the trunk on the thigh • Medially rotates the thigh.
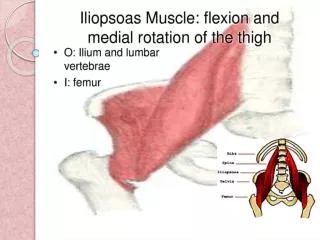
Psoas • A long fusiform muscle that arises within the abdomen and descends into the thigh. • Origin: • From the 12th thoracic to the 5th lumbar vertebrae • From the roots of the transverse processes, • The sides of the vertebral bodies • The intervertebral discs, • Insertion: • The fibers run downward and laterally • Leave the abdomen to enter the thigh by passing behind the inguinal ligament. • The iliopsoas tendon is attached to the lesser trochanter of the femur. • A bursa intervenes between the tendon and the hip joint • May communicate with the joint. • Nerve supply: • Branches from the lumbar plexus. • Action: • The iliopsoas flexes the thigh on the trunk at the hip joint • If the thigh is fixed, it flexes the trunk on the thigh.
Psoas minor • The psoas minor is a long, slender skeletal muscle which, when present, is located in front of the psoas major muscle • This muscle does not exist in About half the human population Origin • From sides of vertebrae T12 and L1, I.V. discs and transverse processes • Insertion • To superior ramus of pubic bone (pectineal line). • Action • It is a weak muscle and has no significant role in human body. • It acts as a weak flexor of the lumbar vertebral column. Nerve supply • Anterior primary rami of L1
Psoas Muscles Psoas major muscle Psoas minor muscle
Pectineus • Origin: • From the superior ramus of the pubis • Insertion: • The muscle fibers pass downward, backward,and laterally • Attached to the upper end of the linea aspera just below the lesser trochanter. • Nerve supply: • Femoral nerve • Occasionally, it receives a branch from the obturator nerve • Action: • Flexes and adducts the thigh at the hip joint
Quadriceps Femoris • The quadriceps femoris muscle consists of four parts: • Rectus femoris • Vastus lateralis • Vastus medialis • Vastus intermedius • A common tendon of insertion into the upper, lateral, and medial borders of the patella • Via the ligamentum patellae, into the tubercle of the tibia.
Rectus Femoris • Origin: • A straight head from the anterior inferior iliac spine • A reflected head from the ilium above the acetabulum • Insertion: • The two heads unite in front of the hip joint, • The bipennate muscle is inserted into the quadriceps tendon and so into the patella. • Nerve supply: • Femoral nerve
Vastus lateralis • Origin: • From the intertrochanteric line • The base of the great trochanter • The linea aspera of the femur • Insertion: • The fibers pass downward and forward to be inserted into the quadriceps tendon and so into the patella. • Some of the tendinous fibers join the capsule of the knee joint and strengthen it. • Nerve supply: • Femoral nerve
Vastus Medialis • Origin: • From the intertrochanteric line • the linea aspera of the femur • Insertion: • The fibers pass downward and forward • inserted into the quadriceps tendon and so into the patella. • Some of the tendinous fibers join the capsule of the knee joint and strengthen it. • The lowest muscle fibers are almost horizontal in direction and prevent the patella from being pulled laterally during contraction of the quadriceps muscle. • Nerve supply: • Femoral nerve
Vastus Intermedius • Origin: • From the anterior and lateral surfaces of the shaft of the femur • Insertion: • The fibers pass downward • join the deep aspect of the quadriceps tendon. • Nerve supply: • Femoral nerve • The articularis genus • a small part of the vastus intermedius • inserted into the upper part of the synovial membrane of the knee joint. • It serves to retract the synovial membrane superiorly during extension of the knee joint.
Action of Quadriceps Femoris Muscle (Quadriceps Mechanism) • a powerful extensor of the knee joint. • Some of the tendinous fibers of the vastus lateralis and vastus medialis form bands, or retinacula, that join the capsule of the knee joint and strengthen it. • The lowest muscle fibers of the vastus medialis are almost horizontal and prevent the patella from being pulled laterally during contraction of the quadriceps muscle. • The tone of the quadriceps muscle greatly strengthens the knee joint. • The rectus femoris muscle also flexes the hip joint.
QUADRICEPS FEMORIS AS A KNEE JOINT STABILIZER • The quadriceps femoris is a most important extensor muscle for the knee joint. • Its tone greatly strengthens the joint • Carefully examined • Both thighs should be examined • Size • Consistency • Strength • Reduction in size caused by muscle atrophy can be tested by measuring the circumference of each thigh a fixed distance above the superior border of the patella. • The vastus medialis muscle extends farther distally than the vastus lateralis. • The vastus medialis is the first part of the quadriceps muscle to atrophy in knee joint disease and the last to recover.
RUPTURE OF THE RECTUS FEMORIS • The rectus femoris muscle can rupture in sudden violent extension movements of the knee joint. • The muscle belly retracts proximally, leaving a gap that may be palpable on the anterior surface of the thigh. • In complete rupture of the muscle, surgical repair is indicated. • RUPTURE OF THE LIGAMENTUM PATELLAE • This can occur when a sudden flexing force is applied to the knee joint when the quadriceps femoris muscle is actively contracting.
Femoral sheath • a funnel- shaped sheath , derived from transversalis fascia anteriorly and iliac fascia posteriorly. • It surroumds the femoral vessels and lymphatic about 2.5cm blow to the inguinal ligament. • Its lower end disappears at the lower margin of the saphenous opening where the sheath fuses with the adventitia of the vessels.
Femoral a. Femoral v. Femoral ring • The femoral sheath is divided into three compartments by two fibrous septa. • The femoral artery occupies the lateral compartment of the sheath. • The femoral vein lies the middle compartment. • The medial compartment is small, called the femoral canal.
Femoral a. Femoral v. Femoral ring The femoral canal • It is about 1.3cm long • its upper opening is called the femoral ring . • The boundaries of the femoral ring are: • the inguinal ligament, anteriorly • the lacunar ligament, medially • the pecten of pubis, posteriorly • the femoral vein, laterally. • covered by femoral septum superiorly.
TheFemoral Canal • Contains: • Fatty connective tissue • All the efferent lymph vessels from the deep inguinal lymph nodes • One of the deep inguinal lymph nodes.
TheFemoral Canal • The femoral sheath is adherent to the walls of the blood vessels and inferiorly blends with the tunica adventitia of these vessels. • The part of the femoral sheath that forms the medially located femoral canal is not adherent to the walls of the small lymph vessels • It is this site that forms a potentially weak area in the abdomen.
FEMORAL SHEATH AND FEMORAL HERNIA • Femoral hemia • A protrusion of peritoneum could be forced down the femoral canal, pushing the femoral septum before it. • The hernial sac descends through the femoral canal within the femoral sheath. • More common in women than in men (possibly because of their wider pelvis and femoral canal). • The hernial sac passes down the femoral canal, pushing the femoral septum before it. • It expands to form a swelling in the upper part of the thigh deep to the deep fascia • With further expansion, the hernial sac may turn upward to cross the anterior surface of the inguinal ligament.