Download
1 / 82
840 likes | 1.17k Views
Alcohol, Tobacco, and Other Drugs. Sara Kossove, LCSW Psychotherapist 201-674-3800 skossove@hotmail.com. Today We Will Discuss… . Personal Attitude About Addiction. Stigma, Moral vs. Medical Model Symptoms of Addiction and Relapse Withdrawal and Tolerance The Addicted Brain

E N D
Alcohol, Tobacco, and Other Drugs Sara Kossove, LCSW Psychotherapist 201-674-3800 skossove@hotmail.com
Today We Will Discuss… • Personal Attitude About Addiction. Stigma, Moral vs. Medical Model • Symptoms of Addiction and Relapse • Withdrawal and Tolerance • The Addicted Brain • Assessment and Diagnosis • Summary of Bergen County Data • Depressants • Anxiolytics / Benzodiazapenes • Opiate Replacement Therapies: Methadone and Suboxone • Treatment for Alcohol, Tobacco and Drugs • Community Resources
Uncover Your Personal Attitude About Addiction Stigma Moral vs. Medical Discrimination Non-Judgmental Respectful Caring
What Are Your Values? • Education? • Trust? • Loyalty? • Family? • Honest Communication in relationships?
Moral vs. Disease (Medical) Models • Moral Deficiency? Character Flaw? Behavioral Mismanagement OR • Disease of Addiction? Complete abstinence, Zero Harm Reduction
Disease Model • Biological model • Downplays importance of understanding etiology • Ignores predisposing psychological vulnerabilities • Deals with distortions of personality and behavior as consequences, not causes of addiction • The more severe the addiction, the better the disease model fits • 12-step programs can and do promote lasting changes in behavior and personality, but usually only for those who remain meaningfully involved and truly “work the program” over the long term
Social Work Values Creating a welcoming, safe environment for clients incorporating values of dignity and worth of the person is vital in assessing and treating individuals with substance use disorders.
Social Work Code of Ethics Service Social Justice Importance of Human Relationships Integrity Competence Dignity and Worth of the Person
Social Work Code of Ethics Professional Competence is crucial in order for clients to get what they need from the Health Care Professional. Social workers practice within their areasof competence and develop and enhance their professional expertise. Do not hesitate for refer to an addiction professional. Ask the licensed practitioner where they have been trained.
From your classmate to the Town Business Administrator, addicts come from various walks of life. Given that addiction does not discriminate, being non-judgmental will travel a long way in a substance abuse assessment. What Does An Addict Look Like?
What Is Addiction? • Addiction is a chronic, but treatable disorder. People who are addicted cannot control their need for alcohol or other drugs, even in the face of negative health, social or legal consequences.
What Is Addiction? • Substance use disorders travel along a continuum. In other words, addiction does not occur overnight. For most people, a progression takes place that involves a series of steps from experimentation and occasional use [to] the actual loss of control of use. This process defines addiction.The progression of addiction can be measured by the amount, frequency and context of a person's substance use.
Psychological factorsand Addiction • There is a strong connection between adverse childhood experiences (various types of physical and psychological trauma) and later development of addictive disorders • Mood and other psychiatric disorders are neither necessary or sufficient to cause addiction. • Alleviating psychiatric symptoms with medication does not prevent relapse to substance use • Addiction is not in the drug. It is in the person using the drug
Symptoms of Addiction • Tolerance Symptoms of addiction include tolerancewhich is the development of resistance to the effects of substance over time. • Withdrawal Symptoms of addiction also include withdrawal which is an unpleasant often painful physical, emotional, psychological response when the substance is discontinued or withheld.
Symptoms of Addiction (Cont’d) • Many people deny that they are addicted. They often emphasize that they enjoy drinking or taking other drugs. This is also known as glorification. • As their illness deepens, addicted people need more of the substance; they may use more often, and use in situations they never imagined when they first began to drink or take drugs. The illness becomes harder to treat and the related health problems, such as organ disease, become worse.
Symptoms of Addiction (Cont’d) • People recovering from addiction can experience a lack of control and return to their substance use at some point in their recovery process. This faltering, common among people with most chronic disorders, is called relapse. • To ordinary people, relapse is one of the most perplexing aspects of addiction. To most addiction providers, it is often viewed as part of the recovery process.
Using to Survive • Just as food and water are linked to our survival in day-to-day living, drugs begin to take on the same significance for addicts. • The need to obtain and take drugs becomes more important than any other need, including truly vital behaviors like eating. • Rather than spending money on food, the addict will spend their entire paycheck on obtaining their substance. • Eventually, the drive to seek and use the drug is all that matters, despite devastating consequences.
Relapse: Part of Addiction as a Chronic Disease Health Care Professionals may observe what is commonly described as a “revolving door” to treatment. This refers to the continuous cycle of re-entry into treatment (detox, inpatient rehabilitation, Emergency Rooms or physician’s offices). Often referred to as, “frequent flyers” or “repeat offenders” individuals often enter treatment multiple times before entering recovery.
Relapse • Relapse is a challenge to achieving sustained recovery. • People trying to recover from drug abuse and addiction are often doing so with altered brains, strong drug-related memories and diminished impulse control. • Accompanied by intense drug cravings, these brain changes can leave people vulnerable to relapse even after years of being abstinent.
Relapse (Cont’d) • Relapse happens at rates similar to the relapse rates for other well-known chronic medical illnesses like diabetes, hypertension and asthma. • Just as an asthma attack can be triggered by smoke, or a person with diabetes can have a reaction if they eat too much sugar, a drug addict can be triggered to return to drug abuse.
The Addicted Brain • A person takes any drug, brain pleasure circuits are activated. • Surge in levels of dopamine, which results in feelings of pleasure. The brain remembers this pleasure and wants it repeated.
Brain Changes • Reduced dopamine activity. • Drugs produce very large and rapid dopamine surges and the brain responds by reducing normal dopamine activity. • Eventually, the disrupted dopamine system renders the addict incapable of feeling any pleasure even from the drugs they seek to feed their addiction.
Brain Changes(Cont’d) • Altered brain regions that control decision making and judgment. Drugs of abuse affect the regions of the brain that help us control our desires and emotions. The resulting lack of control leads addicted people to compulsively pursue drugs, even when the drugs have lost their power to reward.
The Brain's Pleasure Pathway: Beyond Willpower Addiction can develop despite a person's best intentions and in spite of their strength of character. Repeated drug use disrupts complex but well balanced systems in the human brain. Many people are addicted to more than one substance, complicating their efforts to recover.
1,294 individuals (7.3%) were admitted for ALCOHOL 340 Individuals (5.1%) admitted for COCAINE 709 individuals (3.1%) admitted for HEROIN / OPIATES 384 individuals (4.8%) admitted for MARIJUANA 93 individuals (3.6%) admitted for OTHER substance 2,820 individuals (4.9%) of the State’s total were from Bergen County Bergen County Admissions to Substance Abuse Treatment (Bergen County Overview, Division of Addiction Services, 2007).
How Addiction is Diagnosed … Addiction is diagnosed through structured assessment and use of a diagnostic code from the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM IV).
DSM IV Multiaxial Assessment: • AXIS I Clinical Disorders • AXIS II Personality Disorders Mental Retardation • AXIS III: General Medical Conditions • AXIS IV: Psychosocial and Environmental Problems • AXIS V: Global Assessment of Functioning (GAF)
Assessment:What Do We Measure ? • Etiology • Course • Severity • Client readiness • Relationship of alcohol and other life problems • Strengths, resources • Relapse risk
Importance of Assessment Assessment means that you as the interviewer are responsible for the integrity of the information collected and “must be willing to repeat, paraphrase, and probe until he/she is satisfied that the patient understands the questions and that the answer reflects the best judgment of the patient, consistent with the intent of the question.” (ASI Manual)
Quantity/Frequency Screen 1. “Do you drink alcohol?” 2. “On average, how many days a week do you drink?” 3. “On a day when you drink alcohol, how many drinks do you have?” 4. “What is the maximum number of drinks you consumed on any given occasion in the past month?” 8 or more drinks/week or 2 or more occasions of binge drinking in last month are indicative of alcohol use problems.
Alcohol -Induced Diagnoses • 305.00 Alcohol Abuse • 303.90 Alcohol Dependence • 291.8 Alcohol Withdrawal
Diagnostic Criteria:Alcohol Abuse • Maladaptive pattern of use leading to clinically significant impairment or distress. • Symptoms never met criteria for dependence • Intentional overuse of alcohol (celebration, anxiety, despair, self-medication, or ignorance resulting in…
Alcohol Abuse (Cont’d) 1+ of the following within a 12-month period… • Failure to fulfill major role obligations • Recurrent drinking is physically hazardous • Continued alcohol use despite persistent or recurrent problems • Recurrent alcohol-related legal problems
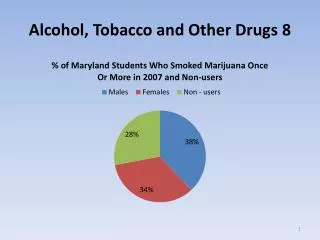
The Drug of Choice Among Adolescents • Three-fourths of 12th graders, more than two-thirds of 10th graders, and about two in five 8th graders have consumed alcohol (more than a few sips) in their lifetime. Forty-five percent of 12th graders; 34 percent of 10th graders; and 17 percent of 8th graders reported using alcohol in the past month – more than cigarettes and marijuana combined. • Underage Drinking is Widespread: There are an estimated 10.8 million underage drinkers in the U.S.
Diagnostic Criteria:Alcohol Dependence • Characterized by impaired control of alcohol use during intoxication and/or inability to abstain from drinking despite consequences. • Tolerance:need for increased amounts to achieve desired effect or diminished effect with same amount • Withdrawal:Tremors, Sweats, Nausea, Anxiety, Sleep disturbance, Hallucination, Seizure
Alcohol Dependence (Cont’d) • Persistent desire to drink • 1+ unsuccessful attempts to cut down • Drinking more than intended • Giving up important activities because of drinking • Spending a great deal of time obtaining alcohol • Needing to drink to recover from alcohol effects
Alcohol Dependence vs. Abuse • Alcohol dependence with partial remissiondiffers from alcohol abuse • Current diagnostic criteria may be the same, but a past history of dependence is important and relevant --- it has different implications for both the future and treatment
Diagnostic Criteria:Alcohol Withdrawal • Cessation of (or reduction in) alcohol use that has been heavy and prolonged. • Two or more of the following, developing within several hours to a few days after reduction in drinking: • Autonomic hyperactivity (sweating, or pulse rate greater than 100). • Increased hand tremor • Insomnia • Nausea or vomiting • Transient visual, tactile, or auditory hallucinations or illusions • Psychomotor agitation • Anxiety • Grand mal seizures
DSM-IV Limitations • Over-reliance on clinician judgment • Diagnostic criteria are less valid with certain populations • Does not capture levels of drinking involvement • Provides little help with motivation or treatment planning
Case Example • 23 year old male law student with no prior treatment history was referred by the local Intoxicated Drivers Resource Center for a DUI. He reported binge drinking (15 beers) on the night of his DUI and states he often drinks this way on weekends / at college parties. He reports a family history of alcoholism and states he has continued to drink since the DUI. What is his diagnosis?
Anxiolytics/Benzodiazepines • Benzodiazepines are widely abused by addicts and are often prescribed for a variety of conditions, particularly anxiety. • Physicians often prescribe this for detoxification from alcohol. Alone, they are relatively safe and, with overdose, rarely result in death. • However, used chronically, or in combination with other substance specifically alcohol, benzodiazepines are highly addicting,cause toxicity and could result in death. • Psychiatrists need to use alternatives to benzodiazepines such as antidepressants, anticonvulsants, buspirone, and others.
Opiates We have a growing opiate epidemic in Bergen County.
Oxycodone Percocet Vicodin Heroin Roxicet Fentanyl Morphine Codeine Tylenol with Codeine Opium Hydrocodone Hydromorphone Darvocet Percodan Tylox Methadone Suboxone Commonly Abused Opiates
Heroin Methods of use: • Intravenous injection (IV) • Intranasal (snorting) • Smoking by inhaling its vapors when heated, i.e. "chasing the dragon.” • Smoking results in an almost immediate effect that builds in intensity.
Heroin • Onset of heroin's effects depends upon the route of administration. • IVuse induces a rush and euphoria usually taking effect within 30 seconds; intramuscular and subcutaneous injection take effect within 3 to 5 minutes. • Snorting results in an onset within 3 to 5 minutes.
Heroin • A first-time user typically ingests between 5mg and 20 mg of heroin. • Heavily dependent users may require several hundred mg per day. • IV drug users are at serious health risks due to the use of unsterile needles: • the risk of contracting blood-borne pathogens such as HIV and hepatitis • abscesses
Effects of Heroin Use • The short-term effects of heroin abuse appear soon after a single dose and disappear in a few hours. • After an injection of heroin, the user reports feeling a surge of euphoria ("rush") accompanied by a warm flushing of the skin, a dry mouth, and heavy extremities. • Following this initial euphoria, the user goes "on the nod," an alternately wakeful and drowsy state. • Mental functioning becomes clouded due to the depression of the central nervous system.