Download
1 / 58
590 likes | 936 Views
Microbiology 2011 5/6/2011 Yu Chun-Keung DVM, PhD . Miscellaneous Small Gram-Negative Bacilli Chapter 34 Haemophilus Chapter 35 Bordetella Chapter 36 Francisella Brucella. Chapter 34 Haemophilus. Family Pasteurellaceae

E N D
Microbiology 2011 5/6/2011 Yu Chun-Keung DVM, PhD MiscellaneousSmall Gram-Negative Bacilli Chapter 34 Haemophilus Chapter 35 Bordetella Chapter 36 Francisella Brucella
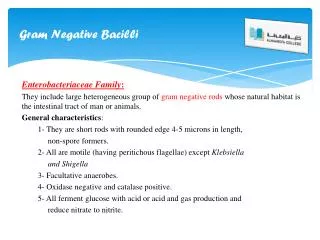
Chapter 34 Haemophilus Family Pasteurellaceae Genera Haemophilus Actinobacillus Aggregatibacter Pasteurella Small, G(-), non-spore-forming bacilli Fastidious growth needs
Genus Haemophilus 嗜血桿菌 • “Blood-lover” • Growth require hemin (x factor) and nicrotinamide adenine dinucleotide, NAD (vfactor) • Heated blood (chocolate) agar for isolation • Important Haemophilius species • H. influenzae (an important pathogen) • H. ducreyi (soft chancre) • H. aegyptius (acute, purulent conjunctivitis) • H. parainfluenzae (rarely pathogenic)
Classification H. influenzae(Hi) • Many but not all strains is covered with polysaccharide capsule Serological differentiation - capsular antigens: serotype a to f • Biochemical properties - indole production, urease activity, ornithine decarboxylase activity : biotypeI to VIII
Pathogenesis Non-encapsulated Hi &H. parainfluenzae(non-typeable) • Colonize URT in all people • 10% of the flora of saliva: H. parainfluenzae • Opportunistic pathogens: spread locally and cause acute and chronic otitis, sinusitis, bronchitis, and pneumonia.
Pathogenesis - encapsulated Hi type b • Uncommon in the URT • Common cause of disease in unvaccinated children • Invasion: adhesins colonization of oropharynx release cell wall components damage and impair ciliary function across epithelial and endothelial cells blood • Produce IgA1 proteases, facilitate colonization • LPS lipid A induces meningeal inflammation
Major virulence factor: antiphagocytic polysaccharide capsule –polyribitol phosphate (PRP) : ribose, ribitol, phosphate • Natural infection, vaccination, passive transfer of material antibody - anti-PRP antibody is protective (enhance phagocytosis and complement-mediated bacteriocidal activity) • Absence of anti-PRP antibody (complement depletion, splenectomy ) leads to invasion, bacteremia and dissemination Phagocytic engulfment of H. influenzae bacterium opsonized by antibodies specific for the capsule and somatic (cell wall) antigen. 2004 Kenneth Todar University of Wisconsin-Madison Department of Bacteriology
Clinical diseases (Hib infection) • Meningitis: Hi type b was the most common cause of pediatric meningitis (3 -18 m). Age-specific incidence of bacterial meningitis caused by Haemophilus influenzae, Neisseria meningitidis and Streptococcus pneumoniae prior to 1985 2004 Kenneth Todar University of Wisconsin-Madison Department of Bacteriology
Clinical diseases (Hib infection) • Epiglotitis 會厭炎: 2-4 yrs; swelling of the supraglottic tissue, pharyngitis, fever, rapidly progress to complete obstruction of the airways, life-threatening emergency. • Cellulitis 蜂窩織炎: fever, reddish-blue patches on the cheeks or periorbital area. • Arthritis: the most common form of arthritis (single large joint) in children <2 yrs.
Transmission • Person-to-person transmission in non-immune population • Increased disease frequency in households where there is a primary case or an asymptomatic carrier. • Primary risk factor for invasive disease = absenceof anti-PRP antibody. • Close contacts should be given chemoprophylaxis.
Diagnosis • Clinical diagnosis • History, physical examination • Sign: are those findings that a physician can objectively detect or measure. • Symptom: are those problems that a patient notices or feels. • Laboratory diagnosis • detection / identification of pathogens (i.e., whole cell, protein, nucleic acid) • detection of immune responses (i.e., antibodies)
Diagnosis • Specimens: • Oral swab: avoid contamination with oral secretions • Sputum from LRT • Direct needle aspiration • Cerebrospinal fluid (CSF) and blood (>107 bacteria/ml) • Microscopy: both sensitive & specific; G(-) bacilli in CSF in >80% cases before antibiotics treatment
Diagnosis (for Hib only) • Particle agglutination test : • Detect PRP antigen, rapid and sensitive (1 ng/ml) • Anti-PRP Ab-coated latex particles + specimen, if PRP present, “positive” agglutination • Culture: • Chocolate agar, colony 1-2 mm. • Blood agar: Hib grows around colonies of Staph. aureus on blood agar - Satellite phenomenon
Treatment • Prompt antimicrobial therapy for systemic Hib infections, otherwise mortality 100% • Serious infections: cephalosporins Less severe infections (otitis, sinusitis): ampicillin • Antibiotic chemoprophylaxis (rifampin) for high risk group (children < 2ys with patients around)
Prevention • Polysaccharide vaccine for Hib were not effective for children < 18m (the high risk population). • Hi type b conjugate vaccine • Purified capsular PRP + Carrier proteins: Meningococcal outer membrane protein Diphtheria toxoid Tetanus toxoid
Before the introduction of conjugated vaccine, Hibwas a common pediatric disease in children < 5 yrs. • Hib conjugate vaccine was introduced in 1987 which greatly reduced the incidence of disease (> 90%).
Epidemiology • Now Hib infections only occur in nonimmune children or adults with waning immunity. • Other serotypes of encapsulated strains and non-encapsulated strains become more common. • Hib remains a significant pediatric pathogen worldwide, especially in developing countries.
Haemophilus ducreyi • A sexually transmitted disease; most common in Africa and Asia • Painful ulcer on genitalia (soft chancre, 軟性下疳)with regional lymphadenopathy • Differential: • Syphilis; Herpes simplex; Lymphogranuloma venereum (caused by Chlamydia trachomatis)
Genus Aggregatibacter • A. actinomycetemcomitans and A. aphrophilus • Mouth flora blood damaged heart valve / artificial valve subacute endocarditis • Difficult to diagnosis : develop slowly and the bacteria grow slowly in blood agar (> 5 days)
Genus Pasteurella • P. multocida and P. canis • Primarily animal pathogen. • Commensals in oropharynx of health animals. • Human infections result from animal contact (bites, scratches, shared food). • The most common organism in human wounds inflicted by bites from cats and dogs.
Three general forms of disease • Localized cellulitis and regional lymphadenopathy after animal bite or scratch. • Exacerbation of chronic respiratory tract disease in patients with underlying pulmonary dysfunction. • Systemic infection in immunocompromised patients.
Lab diagnosis • Grows well on blood and chocolate agar • Large, buttery colonies with a musty odor Treatment • Susceptible to a variety of antibiotics • Penicillin, macrolides, tetracycline …
Chapter 35Bordetella • Extremely small (0.2 x 1 μm ), G(-), coccobacilli • Have simple nutritional requirement • Some species (i.e., B. pertussis) are highly susceptible to toxic substances and metabolites in media (need charcoal, starch, blood, or albumin to absorb toxic substances)
Important Bordetella species • B. pertussis: whooping cough / pertussis (severe cough) B. parapertussis: mild form of pertussis B. bronchiseptica: respiratory disease of animals (pigs and dogs) B. holmesii: uncommon cause of sepsis • The four species are closely related, differing only in the expression of virulence genes
Pathogenesis • Exposure (aerosol) • Attachment to ciliated epithelial cells of the respiratory tract by means of adhesins(黏附因子) • Proliferation • Production of toxins • Localized tissue damage and systemic toxicity Colonization of tracheal epithelial cells by Bordetella pertussis 2004 Kenneth Todar University of Wisconsin-Madison Department of Bacteriology
Bacterial adhesins • Filamentous hemagglutinin: contain RGD motif: bind (1) sulfated glycoprotein integrins on ciliated respiratory cells; (2) CR3 on macrophages, and trigger phagocytosis without initiating oxidative burst (intracellular survival, escape from Ab) • Pertactin : contain RGD motif • Fimbria : mediate binding in vitro; in vivo function unknown • Pertussis toxin:A classic A-B toxin with a toxic subunit (S1) and binding subunits (S2 to S5); S2 binds lactosylceramide on ciliated respiratory cells, S3 binds phagocytic cells
Toxins • S1 subunit of pertussis toxin • Adenylate cyclase toxin / hemolysin • Dermonecrotic toxin • Tracheal cytotoxin • LPS
S1 subunit of pertussis toxin S2-S5 binding subunit S1 toxic subunit Adenosine diphosphate-ribosylating activity for G protein, which regulates adenylate cyclase activity (convert ATP to cAMP). Increase respiratory secretion and mucus production.
Tracheal cytotoxin: (1) target ciliated epithelial cell; ciliostasis, extrusion of ciliated cells, impair regeneration of damaged cells by interfering DNA synthesis (disrupt clearance mechanism, lead to cough); (2) IL-1 production (lead to fever) A tracheal organ culture 72 h after infection with B. pertussis. Large arrow: Bordetella Small arrow: cilia Extruded epithelial cell with attached bacteria Denuded epithelium Normal ciliated epithelial cell
Toxins • Adenylate cyclase toxin / hemolysin: (1) activated by calmodulin and converse ATP to cAMP, increase respiratory secretion; (2) inhibit leukocyte functions • Dermonecrotic toxin: vasoconstriction and tissue destruction • LPS: unknown (activate complement and stimulate cytokine release)
Clinical disease • Infect ciliated epithelial cells of the airways, produce disease locally, no invasion. • Catarrhal phase: resemble common cold, sneezing, serous rhinorrhea, malaise, low-grade fever, 1-2 wk, infectious (disease not recognized with high number of bacteria produced) • Paroxysmal phase: a series of repetitive coughs followed by inspiratory whoop, vomiting, and exhaustion, 40-50 paroxysms daily, lymphoctyosis, 2-4 wk. • Convalescent phase: paroxysms diminish with secondary complications, lasts for above 3 wk.
Clinical disease • Classic presentation may not be seen in patients with partial immunity. • Only chronic persistent cough without whooping or vomiting • Differential diagnosis • Mycoplasma pneumoniae • Chlamydophilia pneumoniae • Legionella pneumophila
Epidemiology • Pertussis was considered a pediatric disease (< 1 year) • Incidence (morbidity and mortality) has been reduced considerably after the introduction of vaccine in 1949. • Still endemic worldwide with a dramatic increase in recent year • Majority of infections are found in adolescents and adults (reason not known).
Lab diagnosis – specimen collection and transport • Extremely sensitive to drying, do not survive outside the host or traditional transport medium. • Inoculate (nasopharyngeal aspirate) to freshly prepared medium or transport medium at bedside. • Use synthetic fiber swabs not cotton swabs (fatty acid are toxic to Bp).
Lab diagnosis - microscopy Direct or indirect fluorescent antibody tests for antigen detection Aspirated specimen microscopic slide air-dried heat fixed fluorescent Ab Sensitivity 50% Fluorescein-labeled rabbit anti-Bp Ab Aspirated specimen Direct Fluorescein-labeled anti-rabbit Ig Ab Rabbit anti-Bp Ab Indirect
Lab diagnosis - culture • Regan-Lowe charcoal medium (horse blood, glycerol, peptones). • 35°C, humidified, 7 days, • 50% sensitivity, affected by • Patient factors (stage of illness, use of antibiotics) • Quality of specimen • Transport conditions • Culture methods
.Nucleic acid amplification • Polymerase chain reaction sensitivity 80-100% • No FDA approved test, in-house assay Serology • ELISAfor antibodies against filamentous hemagglutinin or pertussis toxin • No FDA approved test
Treatment • Primarily supportive. Recovery depends on regeneration of ciliated epithelial cells. • Antibiotics (erythromycin) are effective and can reduce duration of clinical course. • However, the illness is usually unrecognized during catarrhal phase (the peak of contagiousness) • Pertussis is highly contagious; prophylaxis for family members of a symptomatic patient.
Vaccination • DTP vaccine (diphtheria toxoid + tetanus toxoid + inactivated whole cell of Bp), 80-85% effective. • DTP vaccine has not been widely accepted because of vaccine-related complications. • DTaP (acellular vaccine) : subunit vaccine D + T + inactivated pertussis toxin, filamentous hemagglutinin, and pertactin or fimbriae.
Pentavalent vaccine– PEDIACEL (Sanofi Pasteur) • purified polyribose ribitol phosphate (PRP) of Hib • covalently bound to 20 µg of tetanus protein 10 µg • 2. pertussis toxoid 20 µg • filamentous haemagglutinin 20 µg • fimbrial agglutinogens 2 + 3, 5 µg; • pertactin 3 µg • 3. diphtheria toxoid 15 Lf • 4. tetanus toxoid 5 Lf • 5. poliovirus type 1 (Mahoney) 40 D-antigen units • poliovirus type 2 (MEF1) 8 D-antigen units • poliovirus type 3 (Saukett) 32 D-antigen units
Chapter 36Francisella and Brucella • Zoonotic pathogens and potential agents of bioterrorism • Very small G(-) coccobacilli, 0.5 1.5 m, • Fastidious, slow growth on culture (>1 week)
Taxonomically unrelated α-Proteobacteria • Brucella • Rickettsia • Ehrlichia γ-Proteobacteria • Francisella • Legionella • Pasteruella • Pseudomonas
Genus Francisella • Francisella tularensis (Tularemia) • F. tularensis subsp. tularensis (type A) • F. tularensis subsp. holarctica (type B) • F. tularensis subsp. Mediasiatica(rare as pathogen) • F. tularensis subsp. Novicida(rare as pathogen) • Francisella philomiragia (uncommon opportunistic pathogen)
EpidemiologyF. tularensis subsp. tularensis • Natural reservoirs and vectors: >200 species of mammals, birds, blood-sucking arthropods • Type A: • North America: lagomorphs (rabbits, hares), cats, biting arthropod • Type B: • Northern hemisphere: rodents, cats • Those exposed to ticks are high risk for infection in endemic areas i.e., hunters, and lab personnel • Infections occur in summer and winter; warm winter + wet summer (increase in tick population) • Actual numbers of infections > reported cases
Pathogenesis • Pathogenic strains possess antiphagocytic capsule; protect bacteria from complement-mediated killing • Intracellular parasite: can survive for prolonged periods in macrophages; inhibit phagosome-lysosome fusion. • IFN-γ- and TNF-α-mediated activation of macrophage is essential for controlling bacterial replication and killing in early stage. • Specific T cell-mediated activation of macrophage is essential for controlling bacterial replication and killing in late stage.
Clinical disease - Tularemia (Rabbit fever / Tick fever) Clinical symptoms and prognosis determined by route of infection • Ulceroglandular form: cutaneous ulcer + swollen LN, most common • Oculoglandular form: painful conjunctivitis + swollen cervical LN. • Typhoidal form: sepsis • Pneumonic form: pulmonary symptoms • Gastrointestinal form: UlcerCutaneous tularemiainfection microbes.historique.net
Lab diagnosis • Specimen collection: highly contagious: able to penetrate through unbroken skin and mucous membrane + aerosols. extremely hazardous for physician and lab workers; wear gloves and perform work in biohazard hood • Microscopy: Grain stain – not practical; direct staining with fluorescent antibody, more sensitive and specific • Culture: not grow in common medium without cysteine (eg. blood agar); use chocolate agar or buffered charcoal yeast extract (BCYE) agar, take a week or longer • Serology: a 4-fold increase in Ab titer during illness or a single titer of 1:160; antibody persist for many years (past or current infection?); cross-reactivity between Brucella and Francisella
T/P/C • Penicillin and cephalosporin are ineffective (produce β-lactamase) • Streptomycin and gentamicin are effective (high toxicity) • Prompt treatment < 1% mortality rate • Wear protective clothes and use insect repellents, avoid reservoirs and vectors • Prophylactic antibiotics for high risk groups • Live-attenuated vaccine : partly protective
Genus Brucella Six species with four species associated with human diseases B. melitensis: goat and sheep (natural host) B. suis: swine, reindeer, caribou B. abortus: cattle, bison B. canis: dog, fox, coyotes

![GRAM NEGATIVE BACILLI- MICRO {ST1]](https://cdn1.slideserve.com/2240310/gram-negative-bacilli-micro-st1-dt.jpg)